Does pleural effusion ever go away on it's own?
The inflammation that occurs with pleurisy can cause pain with breathing and may even cause a large amount of fluid to collect in the pleural sac. Pleurisy can go away on its own or worsen so that fluid has to be drained from around the lungs.
How serious is a pleural effusion?
The seriousness of the condition depends on the primary cause of pleural effusion, whether breathing is affected, and whether it can be treated effectively. Causes of pleural effusion that can be effectively treated or controlled include an infection due to a virus, pneumonia or heart failure.
Will pleural effusion clear on its own?
Pleural effusion has many causes. They include heart failure, pneumonia and other infections, cancer, pulmonary embolism, liver disease, and inflammation of the tissues around the lungs. How is it treated? A minor pleural effusion often goes away on its own without treatment.
What is the prognosis for pleural effusion?
The prognosis of the patient with a pleural effusion depends on the underlying condition. If due to heart failure, cirrhosis, or malignancy, the effusion is likely to recur. However, most patients with a pleural effusion have no long-term sequelae. Malignant effusions may change the staging and subsequent prognosis of the underlying cancer.

What Is Pleural Effusion?
Pleural effusion, sometimes referred to as “water on the lungs,” is the build-up of excess fluid between the layers of the pleura outside the lungs...
What Causes Pleural Effusion?
Pleural effusions are very common, with approximately 100,000 cases diagnosed in the United States each year, according to the National Cancer Inst...
Is Pleural Effusion Serious?
The seriousness of the condition depends on the primary cause of pleural effusion, whether breathing is affected, and whether it can be treated eff...
What Are The Symptoms of Pleural Effusion?
Some patients with pleural effusion have no symptoms, with the condition discovered on a chest x-ray that is performed for another reason. The pati...
How Is Pleural Effusion Diagnosed?
The tests most commonly used to diagnose and evaluate pleural effusion include: 1. Chest x-ray 2. Computed tomography (CT) scan of the chest 3. Ult...
How Is Pleural Effusion Treated?
1. Treatment of pleural effusion is based on the underlying condition and whether the effusion is causing severe respiratory symptoms, such as shor...
What Is Pleural Effusion?
Pleural effusion is fluid buildup in the space between the layers of the pleura. The pleura are thin layers of tissue that form a 2-layered lining...
What Causes Pleural Effusion?
1. Heart failure or other heart and lung problems such as a pulmonary embolism (blockage of a blood vessel in the lungs) 2. Lung infections such as...
What Are The Signs and Symptoms of Pleural Effusion?
You may have no symptoms. A pleural effusion may cause you to cough or feel short of breath. You may breathe faster than usual. You may have mild t...
How Is Pleural Effusion Diagnosed?
Your healthcare provider will examine you and listen to your heart and lungs through a stethoscope. You may need any of the following: 1. Blood tes...
How Is Pleural Effusion Treated?
Treatment depends on the cause of your pleural effusion and how bad your symptoms are. You may need any of the following: 1. Diuretics may help you...
When Should I Contact My Healthcare Provider?
1. You have a fever. 2. Your breathing problems do not go away or get worse. 3. Your pain does not go away or gets worse. 4. You cough up yellow, g...
When Should I Seek Immediate Care Or Call 911?
1. You feel faint, or you cannot think clearly. 2. Your lips or fingernails turn blue. 3. You find it very hard to breathe.
How to remove fluid from pleural membrane?
In a pleural fluid analysis, your doctor will remove fluid from the pleural membrane area by inserting a needle into the chest cavity and suctioning the fluid into a syringe. The procedure is called a thoracentesis. This also works as a common procedure to drain the excess fluid from the chest cavity. The fluid will then be tested ...
What causes pleural effusions?
Other causes of pleural effusions include: congestive heart failure (the most common cause overall) cirrhosis or poor liver function. pulmonary embolism, which is caused by a blood clot and is a blockage in the lung arteries. complications from open-heart surgery. pneumonia.
What causes fluid to accumulate in the chest cavity?
This fluid accumulates in the chest cavity outside the lung, causing what’s known as a pleural effusion.
What is the term for the buildup of fluid in the space between the lungs and chest cavity?
Pleural effusion , also called water on the lung, is an excessive buildup of fluid in the space between your lungs and chest cavity.
What is the treatment for pleural inflammation?
After drawing the excess fluid out of the chest cavity, a doctor injects a drug into the area. The drug is often a talc mixture. This medication causes the two layers of the pleura to stick together, which prevents the future buildup of fluid between them.
What is the first classification of pleural effusions?
The first classification of pleural effusions is either transudative or exudative.
How long does it take for a pleural effusion to go away?
Treatment for some cases of pleural effusion may be managed with medication and other supportive care. Most people recover within a few days or weeks. Minor complications from more invasive treatments can include slight pain and discomfort, which often go away with time. Some cases of pleural effusion can have more serious complications, depending on the severity of the condition, cause, and treatment used.
How to drain fluid from pleural effusion?
This involves inserting a needle in the space between the lung and the chest wall and draining the liquid. In these cases, a doctor may also send a sample of fluid to be tested for other causes, such as lung cancer, for example. Some patients may require a pleural drain that is inserted through the skin so that the buildup of fluid can be drained repeatedly without the need for repeated thoracentesis.
Why do I have pleural effusion?
Pleural effusion occurs when fluid builds up in the space between the lung and the chest wall. This can happen for many different reasons, including pneumonia or complications from heart, liver, or kidney disease. Another reason could be as a side effect from cancer. “One of the most common reasons pleural effusion develops is due to congestive heart failure ,” says Jonathan Puchalski, MD, a pulmonologist at Yale Medicine.
How is fluid around the lung treated?
The best way is to treat the cause of the effusion. If the cause is pneumonia, a doctor will likely prescribe antibiotics to treat the infection, which may also cause the fluid to go away. If fluid build-up has been caused by congestive heart failure, a physician will likely prescribe diuretics, such as Lasix, for treatment.
What are the symptoms of pleural effusion?
The symptoms of pleural effusion can range from none to shortness of breath to coughing, among others. The greater the build-up of fluid, the more likely symptoms will be noticeable. In addition to excess fluid, the tissue around the lung may become inflamed, which can cause chest pain. In extreme cases, a person can have up to four liters of excess fluid in the chest. It's very uncomfortable. “Imagine trying to breathe with two soda bottles pushed up against your lungs,” Dr. Puchalski says.
What makes Yale Medicine’s approach to pleural effusion special?
At Yale Medicine, patients receive care from a team of physicians who specialize in dealing with pleural effusions. The clinical care team includes a physician assistant and an advanced practice registered nurse who are trained in this subspecialty. What makes Yale especially unique, Dr. Puchalski adds, is our ability to perform bilateral thoracenteses. This means that a patient can have fluid build-up removed from both lung areas in a single treatment, rather than scheduling two separate procedures. Patients can do this at Yale Medicine, Dr. Puchalski explains, due to a highly-trained staff.
How much fluid can cause chest pain?
In extreme cases, a person can have up to four liters of excess fluid in the chest. It's very uncomfortable.
Is fluid around the lung dangerous?
Fluid around the lung (pleural effusion) is a potentially dangerous condition that can masquerade as something less worrisome. What may seem like chest pain or coughing due to a bad cold could actually have serious health ramifications. It’s not that rare, either.
How to treat pleural effusion?
Treatment depends on the cause of your pleural effusion and your symptoms. You may need any of the following: Diuretics may help you lose extra fluid caused by heart failure or other problems. Antibiotics help prevent or treat an infection caused by bacteria. NSAIDs help decrease swelling and pain or fever.
How is pleural effusion diagnosed?
Your healthcare provider will examine you and listen to your heart and lungs through a stethoscope. You may need any of the following:
Why do you need surgery for pleural effusion?
Surgery may be needed if your pleural effusion keeps coming back or if it increases your risk for other problems.
What does contrast liquid show on an x-ray?
An x-ray, ultrasound, or CT may show fluid around your lungs, an enlarged heart, or signs of infection. You may be given contrast liquid to help your lungs show up better in the pictures. Tell the healthcare provider if you have ever had an allergic reaction to contrast liquid.
How to get better after lung cancer?
Ask your healthcare provider for information if you need help quitting. Drink liquids as directed and rest as needed. Liquids help to keep your air passages moist and better able to get rid of germs and other irritants.
What is the pleura?
The pleura is a thin piece of tissue with 2 layers. One layer rests directly on the lungs. The other rests on the chest wall. There is normally a small amount of fluid between these layers. This fluid helps your lungs move easily when you breathe.
How to get rid of a lung infection?
Rest when you feel it is needed. Deep breathing and coughing will decrease your risk for a lung infection. Take a deep breath and hold it for as long as you can. Let the air out and then cough strongly. Deep breaths help open your airway. You may be given an incentive spirometer to help you take deep breaths.
How to take fluid from pleural space?
A healthcare professional may take a sample of fluid from the pleural space by inserting a needle between the ribs.
What is a pleural effusion?
Outlook. Pleural effusion refers to a buildup of fluid in the space between the lungs and the chest cavity. It can result from pneumonia and many other conditions. It can also be life threatening. Pleural effusion, or “water on the lung,” can resemble a respiratory infection. The cause is sometimes respiratory, ...
How to drain chest fluid?
To drain the chest, the healthcare professional will insert a tube into the pleural space and allow the fluid to leave the body.
What causes fluid to leak back into the chest?
Transudate effusion. Transudate effusion usually occurs when another condition causes a pressure imbalance in the blood vessels. As a result, fluid leaks back into the chest. The liquid in the effusion will likely consist of compounds from blood plasma.
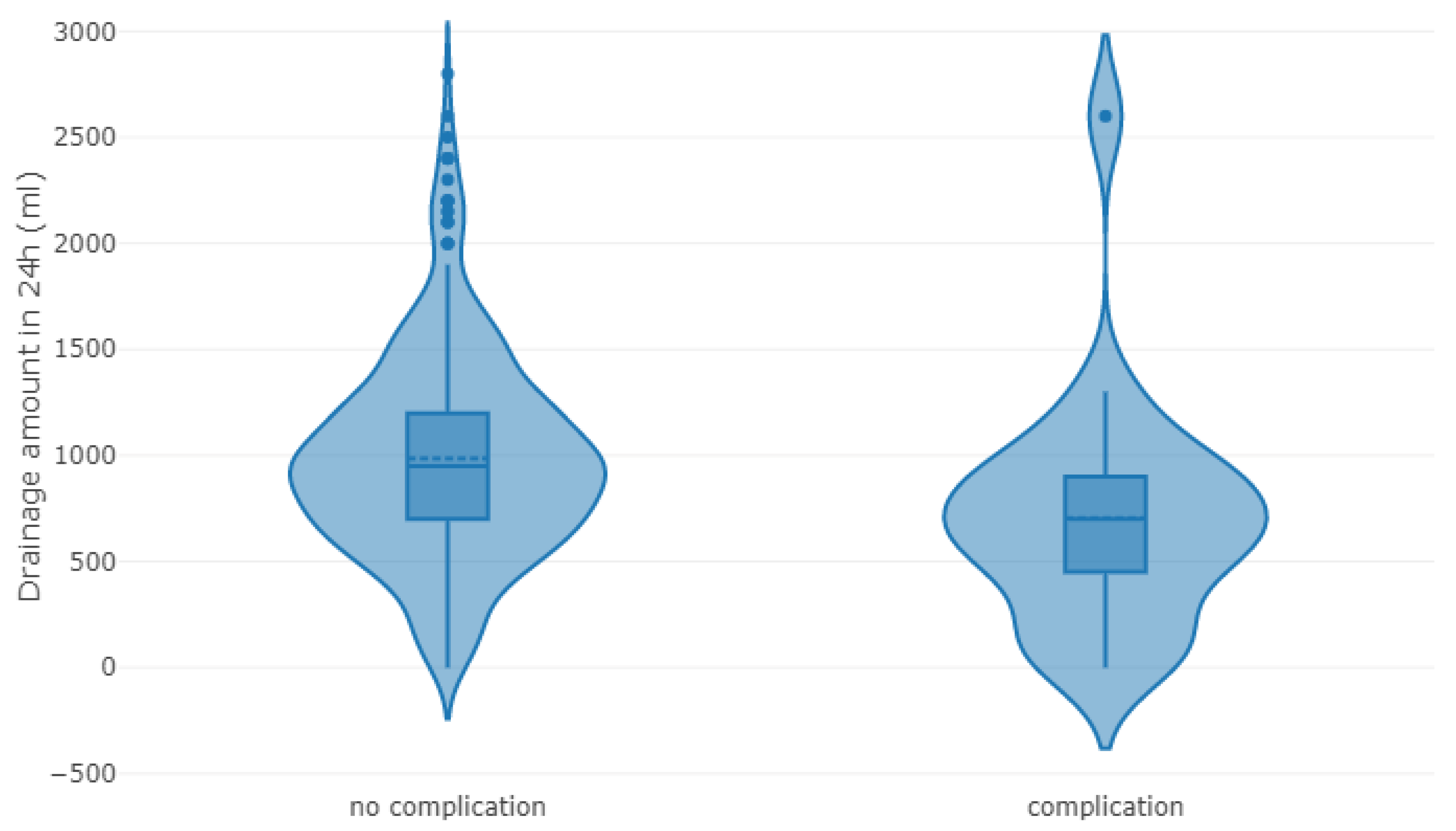
What is the difference between pleural effusion and uncomplicated effusion?
In complicated pleural effusion, signs of inflammation or infection will be present in the fluid. The person may need immediate treatment to prevent potentially serious complications. In uncomplicated effusion, there will be no sign of infection or inflammation in the fluid.
What is the lining of the lungs?
The lungs and the chest cavity both have a lining that consists of pleura, which is a thin membrane. In healthy lungs, these membranes ensure that a small amount of liquid is present between the lungs and chest. This prevents friction as the lungs expand and contract during breathing.
Can pleural effusion be diagnosed?
It can be challenging to diagnose pleural effusion, as the symptoms may overlap with those of many other conditions.
When to clamp pleural tube?
It is necessary to clamp the tube if the patient develops respiratory symptoms (i.e., coughing, chest tightness or pain, shortness of breath or oxygen desaturation) or recommended after draining 1.5 L26. Drainage may be interrupted for up to one hour or more, or until symptoms resolve, and then resumed.
What is the best chest tube size for pleural disease?
However, the Therapeutic Interventions in Malignant Effusion (TIME1) randomized controlled trial found that 12F chest tubes were associated with a higher pleurodesis failure than 24F chest tubes (30% vs. 24%) in 100 patients with malignant effusions, suggesting that chest tube size matters for pleurodesis efficacy12. Moreover, even though the smaller chest tubes resulted in significantly less pain than the larger ones, the difference was not likely clinically significant (mean visual analog scale of 22 vs. 26.8)12. Based upon expert opinion, use of chest tubes ≥20F is recommended in the following situations2,3,5,13: (1) there is clinical concern for the presence of an on-going air leak (or significant risk of it, as in traumatic pneumothorax or bronchial dehiscence), (2) iatrogenic pneumothorax from barotrauma (mechanical ventilation), (3) hemothoraces, and (4) postoperative drainage of the chest cavity.
How is SBCT placed?
SBCT are commonly placed using the catheter-over-guide wire (Seldinger) technique, in which a guide wire is inserted into the pleural space through an introducer needle; the wire should pass without resistance. Then, the needle is removed and dilators are threaded over the wire using a slight twisting action. Afterwards, the chest tube is threaded over the guide wire and into the pleural space, where remains14,17. In cases of pneumothorax, SBCT are directed toward the apex, but for pleural effusions they are directed both inferiorly and posteriorly into the diaphragmatic recess. A silk or synthetic monofilament suture (number 1) along with an adhesive dressing secure the tube in position. An attached 3-way stopcock connects the tube with the drainage system. A chest radiography to confirm the chest tube position is mandatory.
What is a chest tube?
Chest tube insertion is a common procedure usually done for the purpose of draining accumulated air or fluid in the pleural cavity. Small-bore chest tubes (≤14F) are generally recommended as the first-line therapy for spontaneous pneumothorax in non-ventilated patients and pleural effusions in general, with the possible exception of hemothoraces and malignant effusions (for which an immediate pleurodesis is planned). Large-bore chest drains may be useful for very large air leaks, as well as post-ineffective trial with small-bore drains. Chest tube insertion should be guided by imaging, either bedside ultrasonography or, less commonly, computed tomography. The so-called trocar technique must be avoided. Instead, blunt dissection (for tubes >24F) or the Seldinger technique should be used. All chest tubes are connected to a drainage system device: flutter valve, underwater seal, electronic systems or, for indwelling pleural catheters (IPC), vacuum bottles. The classic, three-bottle drainage system requires either (external) wall suction or gravity (“water seal”) drainage (the former not being routinely recommended unless the latter is not effective). The optimal timing for tube removal is still a matter of controversy; however, the use of digital drainage systems facilitates informed and prudent decision-making in that area. A drain-clamping test before tube withdrawal is generally not advocated. Pain, drain blockage and accidental dislodgment are common complications of small-bore drains; the most dreaded complications include organ injury, hemothorax, infections, and re-expansion pulmonary edema. IPC represent a first-line palliative therapy of malignant pleural effusions in many centers. The optimal frequency of drainage, for IPC, has not been formally agreed upon or otherwise officially established.
What is the purpose of a chest tube placement?
Chest tube placement (also called tube thoracostomy) is a common procedure in daily clinical practice which is performed to drain fluid, blood, or air from the pleural cavity. It also serves as a route to instill antibiotics (post-pneumonectomy empyemas), sclerosing agents (pleurodesis), as well as fibrinolytics, DNAse, and/or saline (complicated parapneumonic effusions and empyemas). On the other hand, indwelling pleural catheters (IPC) are becoming a first-line palliative therapy for symptomatic malignant and persistent benign pleural effusions.
Why does my chest tube keep bubbling?
Intermittent or constant bubbling within the water-seal chamber is indicative of an air leak, which is often more apparent when the patient coughs. Causes of bubbling other than a visceral pleural tear include a migrated tube with drainage holes outside the skin, or an inadequate closure of the chest tube insertion site. Moreover, patency of the chest tube is verified by observing respiratory fluctuations of the fluid in the water-seal chamber when the patient is on gravity drainage; no fluctuation indicates that either the tube is occluded or the lung is completely expanded and has blocked the holes of the chest tube inside the chest cavity. Swinging of the fluid in the collecting tube during respiratory cycles (“tiding”) is also characteristic of a correctly placed chest tube.
What are the indications for an intercostal chest drain?
The most common include pneumothoraces, complicated parapneumonic effusions or empyemas, hemothoraces, bedside pleurodesis, and following cardio-thoracic surgery or thoracoscopic procedures to allow for appropriate lung re-expansion2. Moreover, IPC provide symptomatic relief in patients with large malignant effusions, benign effusions resistant to medical therapies, effusions which failed following an attempted pleurodesis, and effusions associated with unexpandable lungs2.
How to help my mom with pulmonary disease?
If the doctor balks tell them you want a new baseline read. With pulmonary rehab she will start an exercise routine that will benefit her breathing capacity, strengthen the muscles that support breathing and improve her stamina. She will breathe more efficiently and that will help reduce risk factors for other pulmonary infections. Rehab groups are limited in size so that the therapist can keep a close eye on all of the patients. Your local hospital should have a Free Breathers Club which will allow her to continue the exercise she started in PR.
How to help my mom with reduced lung capacity?
Because of your mom’s reduced lung capacity she should qualify for pulmonary rehab (PR). Insist on a new pulmonary function test. If the doctor balks tell them you want a new baseline read. With pulmonary rehab she will start an exercise routine that will benefit her breathing capacity, strengthen the muscles that support breathing and improve her stamina. She will breathe more efficiently and that will help reduce risk factors for other pulmonary infections. Rehab groups are limited in size so that the therapist can keep a close eye on all of the patients.
Why is it important to drain pleural effusion?
However, complete drainage is usually avoided to due to fear of re-expansion pulmonary edema.
How much fluid should be removed during thoracentesis?
It is widespread dogma that no more than 1500 ml of fluid should be removed during thoracentesis. For example, this is recommended in the New England Journal of Medicine procedure video and the British Thoracic Society 2010 guidelines.
Why avoid large volume thoracentesis?
Another argument to avoid large-volume thoracentesis is to reduce the risk of ex vacuo pneumothorax. This occurs if the underlying lung is unable to expand, for example due to bronchial obstruction. Thoracentesis generates a low intrapleural pressure which transiently opens a tiny hole in the lung to allow air into the pleural space (alleviating the “vacuum”). Pneumothorax ex vacuo is a benign phenomenon which rarely enlarges or leads to tension pneumothorax, and generally should not be treated with a chest tube ( Heidecker 2006 ).
How many thoracenteses did Abunasser 2010 study?
Abunasser 2010 performed a retrospective study of 300 thoracenteses (including 95 with removal of 1-2 liters, and 42 with removal of >2 liters). Only one case of radiographic RPE occurred following 2.6 liters removed. This patient was on mechanical ventilation prior to the procedure, and there was no change in oxygenation due to RPE.
What is RPE in pulmonary edema?
Traditional model of reexpansion pulmonary edema (RPE) Traditionally it has been believed that RPE was due to the generation of excessively low intra-pleural pressures pulling fluid into the lung tissue (based on Starling's equation ).
How many thoracenteses were removed in 2004?
Pihlajamaa 2004 performed a retrospective study of 262 thoracenteses (including 29 with removal of over 1500 ml). No episodes of RPE were noted.
Why does fluid removal cause chest pain?
Coughing or pleuritic chest pain during fluid removal are physiologic responses to lung re-expansion and catheter irritation of the pleura. Neither requires termination of the procedure.