by Hermann Feeney II
Published 3 years ago
Updated 2 years ago
Clinical features
Pain out of proportion to other physical findings (requiring increasing analgesic requirement) *: Earliest symptom
B. Young Children
Earlier and more sensitive indicator of Pediatric ACS than neurovascular changes or uncontrolled pain
What causes compartment syndrome?
Another nontraumatic cause of compartment syndrome is intraoperative patient positioning, which is particularly important in orthopedic surgery patients. While patients are under anesthesia, they become unaware of pain that may be caused by prolonged malpositioning.
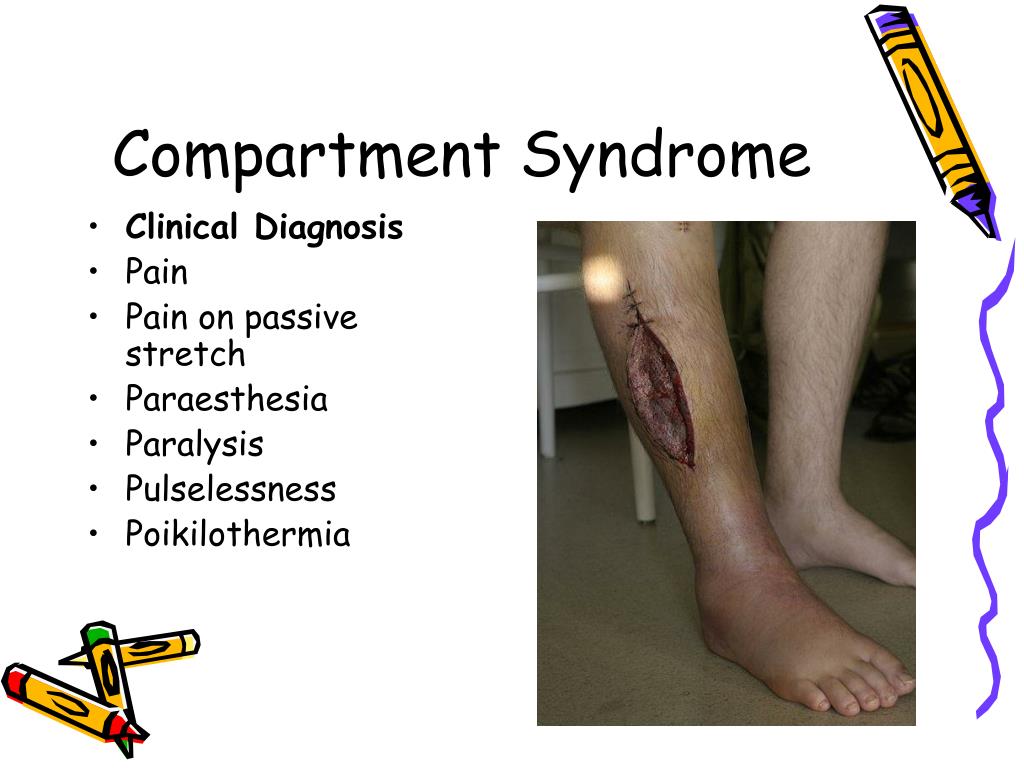
What are the 6 Ps of ACS?
The “6 Ps” (pain , paresthesia, poikilothermia, pallor, pulselessness, and paralysis) are often described as the hallmark findings of ACS, but this is misleading. 4 Pain, especially pain that is disproportionate to the patient's injury or pain that is refractory to pain medication, is the earliest and most common manifestation of ACS. 1,3,9 Distal paresthesia may be present as swelling progresses and nerve conduction is affected but is considered a late finding. Poikilothermia, pallor, pulselessness, and paralysis are considered late findings. 1,3 Although the “6 Ps” are all results of ACS, they cannot be relied on for diagnosis.
What are some examples of ACS?
ACS can be caused by both traumatic and nontraumatic insults. Examples of traumatic causes are fracture, crush injuries, penetrating injuries, burns, and snake bites . Some nontraumatic causes are I.V. infiltration/extravasation, ischemia-reperfusion injury, thrombosis, and hemorrhage. 3 Patients receiving anticoagulants are especially at risk for ACS related to hemorrhage. 3,4,7 In orthopedics, tibial fracture and distal radius fracture are the fractures most commonly associated with ACS. 1-3
What are the compartments of the lower leg?
The lower leg has four discrete compartments: anterior, lateral, deep posterior, and superficial posterior (see Compartments in the lower leg ).
What is ACS in orthopedics?
ACS is a surgical emergency that is most often associated with fracture of the tibia in orthopedics. As a challenging clinical diagnosis, there is significant variation between providers. 30 Delay in diagnosis and treatment can lead to poor outcomes and significant morbidity.
What to expect after fasciotomy?
Following fasciotomy closure, patient education should center around pain control, infection prevention, and regaining function in the affected limb. Most patients will require an assistive device for ambulation and physical therapy postoperatively. 5 Rehabilitation time frames vary, depending on many factors. Weight-bearing status also varies depending on the type of fracture fixation and whether primary soft-tissue coverage was achieved. Orthopedic follow-up is needed for suture removal and serial imaging to confirm fracture alignment and union. After patients have been released from orthopedic care, primary care providers should be aware of the long-term effects of compartment syndrome and fasciotomy. Although there is little risk of recurrent ACS, it has been documented in athletes, which has been attributed to scarring. 5 Common long-term sequelae include chronic pain, persistent neurologic deficits, and dissatisfaction with scarring. 5,29
What is compartment syndrome?
A compartment is a group of muscles, nerves and blood vessels covered by a thin, firm membrane called a fascia. In compartment syndrome, the blood flow, oxygen and nutrients to the muscles and nerves are cut off. Compartment syndrome often occurs in the lower leg but can also affect other parts of the leg, feet, arms, hands, abdomen and buttocks.
What are the different types of compartment syndrome?
Different types of injuries that can cause acute compartment syndrome are. Severely bruised muscle. Major road traffic accident. Crush injury. Fracture. A sudden return of blood flow after circulation gets blocked, such as during surgery. Very tight casts or bandages that are worn for a while.
How to treat acute compartment syndrome?
Treatment of acute compartment syndrome. This requires immediate medical treatment. A surgery called fasciotomy would be required. To relieve pressure, the surgeon makes an incision (cut) through the skin and the fascia, which is the cover of the compartment. After the swelling and pressure go away, the surgeon closes the incision.
19 hours ago
Feb 02, 2022 · Check out the six P’s of compartment syndrome below for warning signs to watch for: 1. Pain. While this is expected with a muscle injury, pain described as deep and constant and poorly localized, that increases when stretching or ... 2. Pallor. If you notice that your patient has pale, shiny skin, ...
5 hours ago
Jun 09, 2020 · What are the 6 Ps of compartment syndrome? The six P's include: (1) Pain, (2) Poikilothermia, (3) Paresthesia, (4) Paralysis, (5) Pulselessness, and (6) Pallor. The earliest indicator of developing ACS is severe pain. Pulselessness, paresthesia, and complete paralysis are found in the late stage of ACS. Click to see full answer.
17 hours ago
Sep 17, 2020 · The 6 Ps of Compartment Syndrome: Episode 119. Use Up/Down Arrow keys to increase or decrease volume. Compartment syndrome occurs when pressure inside a limb or other compartment of the body rises to the point that it impedes blood flow. Left untreated, compartment syndrome can result in tissue death and loss of the affected limb.
28 hours ago
Mar 01, 2018 · The 6 P's of compartment syndrome are: Definition: Paresthesia (numbness/tinling), Pain (distal to the injury & not relieved by opioids 7 pain from passive stretch of affected muscles), Pressure (increases in the compartment), Pallor (coolness and loss of normal color), Paralysis (of affected limb), and Pulselessness (diminished or absent …
33 hours ago
The “6 Ps” (pain, paresthesia, poikilothermia, pallor, pulselessness, and paralysis) are often described as the hallmark findings of ACS, but this is misleading. 4 Pain, especially pain that is disproportionate to the patient's injury or pain that is refractory to pain medication, is the earliest and most common manifestation of ACS. 1,3,9 Distal paresthesia may be present as swelling …
15 hours ago
Diagnosis of ACS is based largely on physical examination and six cardinal clinical manifestations described as the six P's. 1-3, 6, 8 The six P's include: (1) Pain, (2) Poikilothermia, (3) Paresthesia, (4) Paralysis, (5) Pulselessness, and (6) Pallor. 1-3, 8 The earliest indicator of developing ACS is severe pain. Pulselessness, paresthesia, and complete paralysis are found in the late stage of …
28 hours ago
The 6 P's of compartment syndrome STUDY Flashcards Learn Write Spell Test PLAY Match Gravity Created by GTrucc Terms in this set (6) Pain (tenderness) P1... Pallor ( pale skin or poor cap refill) Pain, then.. paresthesia (pins and needles) pain, pallor, then.. pulses (diminished pain, pallor, paresthesia, then.. paralysis
32 hours ago
May 06, 2021 · Acute compartment syndrome: This occurs suddenly and is typically caused by a bad injury, such as a crushing injury. It requires immediate medical attention. If not treated in time, it can permanently damage muscles, cause disability, paralysis or even death. Chronic compartment syndrome: This usually occurs due to physical exertion, such as intense exercise …