What is the electrical axis of the heart?
The electrical axis reflects the average direction of ventricular depolarization during ventricular contraction. The direction of the depolarization ...
What is the normal heart axis?
The electrical axis of the heart (heart axis). As evident from the figure, the normal heart axis is between –30° and 90°. If the axis is more positive than 90° it is referred to as right axis deviation. If the axis is more negative than –30° it is referred to as left axis deviation.
What is the extreme axis deviation of a QRS complex?
Extreme axis deviation (–90°to 180° ): Net negative QRS complex in leads I and II.
What is cardiac axis?
The electrical activity of the heart starts at the sinoatrial node then spreads to the atrioventricular (AV) node.
What is the normal axis of the heart?
Normal cardiac axis. In healthy individuals, you would expect the axis to lie between -30° and +90º. The overall direction of electrical activity is towards leads I, II and III (the yellow arrow below).
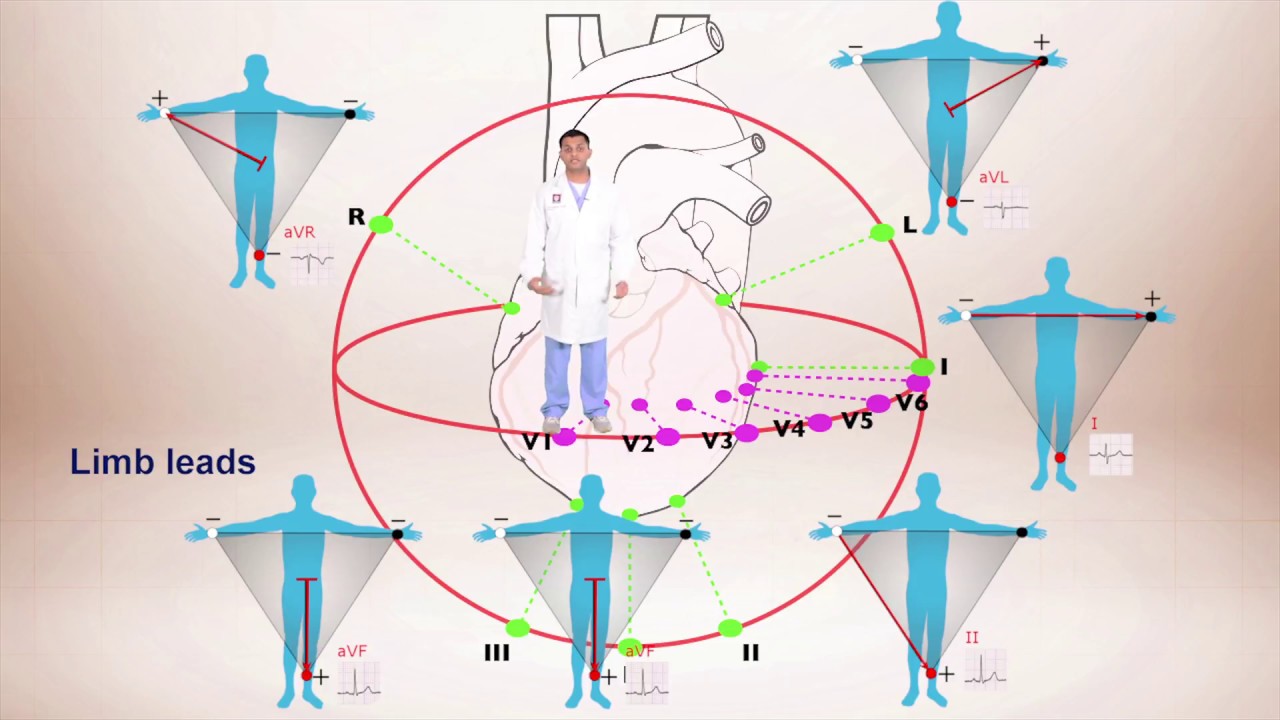
Why does AVR have negative deflection?
You would expect to see the most negative deflection in aVR. This is due to aVR looking at the heart in the opposite direction.
What is the left axis deviation?
Left axis deviation (LAD) involves the direction of depolarisation being distorted to the left (bet ween -30° and -90°).
What gives us an idea of the overall direction of electrical activity?
Whenever the direction of electrical activity is away from a lead you get a negative deflection in that lead. Cardiac axis gives us an idea of the overall direction of electrical activity. Cardiac conduction. Cardiac axis.
Is RAD a condition?
RAD is commonly associated with conditions such as pulmonary hypertension, as they cause right ventricular hypertrophy. RAD can, however, be a normal finding in very tall individuals.
Is RAD a normal finding?
RAD is commonly associated with conditions such as pulmonary hypertension, as they cause right ventricular hypertrophy. RAD can, however, be a normal finding in very tall individuals. Right axis deviation 1.
What does an EKG tell you?
A lot!: For a cardiologist, an EKG can give information about the rate, the rhythm, whether there are signs of a congenital abnormality, signs of a heart attach or blocked artery, the thickness of the heart muscle, previous heart attack, and more. In experienced hands, an EKG can tell an incredible amount of information.
What does Q wave mean in EKG?
Old infarct: A Q wave means an old infarct (a previous heart attack) that result ed in permanent death of a part of the heart muscle. Depending on the location, extent, and other co-morbidities, it may or may not cause new health problems. The Q wave appears because the muscle can no longer transmit electrical signals through the heart. An EKG measures the electrical activity of the heart so that's how it looks.
Is Q wave on EKG normal?
Probably nothing: Q waves of certain width and height on an EKG has been associated with an old heart attack. This hallmark is not very specific and if its boderline and no clinical history or no real cardiac risk factors , its probably a normal variant.
What is the T wave on an ECG?
The axis of the T-wave on the electrocardiogram (ECG) is a marker of ventricular repolarization that, when deviated from normal by more than 60 degrees in either direction in the frontal plane, has been strongly associated with an increased risk of fatal and non-fatal cardiac events in older adults (1) as well as all-cause mortality, incident coronary heart disease (CHD), and death from CHD in older adults free of CHD at baseline (2). Abnormalities in ventricular repolarization on ECG have long been recognized as features of myocardial ischemia. However, the pathophysiologic relationship between CHD and deviation of the T-wave axis from normal is unclear, especially in light of data showing a lack of association between an abnormal T-axis and coronary atherosclerotic disease on angiography (3).
What is abnormal T wave axis?
An abnormal T-wave axis is associated with an increasing CAC score in this population of Icelandic older adults. This association remains in the subgroup of subjects without clinical CHD.
How to calculate frontal T-axis?
Frontal T-axis was calculated by the 12SL program (12). Briefly, the program calculated the signed areas of the T-wave projection in leads I and II by calculating the algebraic sum of samples between the onset and the offset of the T-wave in these leads. The axis was calculated as follows: α = tan−1(2/√3((II-I/2)/I)) where α represents the T-wave axis in the frontal (XY) plane and I and II represent the signed areas of the vectors in leads I and II, respectively. T-wave axis was reported as the angle between the x axis and the axis of the T-wave in the frontal (XY) plane. The main outcome variable used in this analysis was the absolute value of frontal T-axis deviation from 45°. This value was chosen to facilitate comparisons with prior studies in which a frontal T-axis between 15° and 75° was defined as normal (1). QT interval was corrected for rate using Bazett’s equation (QTC= QT interval(msec)/√(60/ventricular rate)). QRS-T angle was derived by subtracting the frontal QRS axis from the frontal T-axis, and the results were divided into gender-specific quartiles based upon an absolute value of the deviation from the population median of 31°. ST-segment depression was defined as Minnesota codes 4.1 or 4.2. Minor ST-segment change was defined as Minnesota codes 4.3 or 4.4. T-wave inversion was defined as Minnesota codes 5.1 or 5.2, and minor T-wave change was defined as Minnesota codes 5.3 or 5.4.
What excludes subjects with CHD or ventricular conduction defects?
Women, excludes subjects with CHD or ventricular conduction defects
What is the name of the machine used to record ECGs?
Resting 12-lead ECGs were recorded using a Marquette/MAC 5000 ECG machine (General Electric Marquette Medical Division, Milwaukee, Wisconsin, USA). Patients were at rest and supine and the electrodes were placed in the standard positions. A technician recorded a 10 second ECG digitized at a rate of 500 samples per second. It was analyzed using the 12 SL analysis program (General Electric Marquette Medical Division, Milwaukee, Wisconsin, USA) and manually by expert readers and coded according to the Minnesota codes (11).
How is CAC quantified?
CAC was quantified using the Agatston method (14). Briefly, in order to calculate an Agatston score, intracoron ary calcified lesions were identified on each slice and a score was computed for each lesion that multiplied the area of the plaque by a factor accounting for tomographic density. These values were summed across all of the slices to create a global score. Gender-specific quartiles of CAC from the entire cohort were used in all analyses.
