
Explore
Treating Asystole Standard asystole treatment involves cardiopulmonary resuscitation, or CPR, and intravenous administration of epinephrine given every three to five minutes as needed. When a reversible underlying cause is found, that cause should be treated directly to reverse asystole. Some theoretically reversible causes of asystole include:
What is the treatment for asystole?
When treating asystole, epinephrine can be given as soon as possible but its administration should not delay initiation or continuation of CPR. After the initial dose, epinephrine is given every 3-5 minutes. Rhythm checks should be performed after 2 minutes (5 cycles) of CPR.
When should epinephrine be given to a patient with asystole?
ACLS Asystole Treatment Algorithm Conduct an initial patient assessment, checking for respirations and pulse If the patient is not breathing and has no pulse, start CPR Establish an airway and administer oxygen to keep oxygen saturation above 94%
What is the ACLS asystole treatment algorithm?
For most patients, true asystole is the result of a prolonged illness or cardiac arrest, and prognosis is very poor. The few patients that have a positive outcome following a diagnosis of cardiac arrest with asystole will usually result from the identification and correction of an underlying cause of the asystole.
What is the prognosis of asystole?
When the patient is in asystole the preferred initial treatment is?
If the initial rhythm is pulseless electrical activity or asystole, an initial dose of epinephrine 1 mg IV/IO (intravenous/intraosseous) should be administered as soon as possible after recognition of cardiac arrest.
What do you do in case of asystole?
Asystole is treated by cardiopulmonary resuscitation (CPR) combined with an intravenous vasopressor such as epinephrine (a.k.a. adrenaline). Sometimes an underlying reversible cause can be detected and treated (the so-called "Hs and Ts", an example of which is hypokalaemia).
What is the ACLS protocol for asystole?
Asystole Case Teaching (ACLS Algorithms) CPR needs to be initiated first. Asystole is not a shockable rhythm and treatment for Asystole involves high quality CPR, airway management, IV or IO therapy, and medication therapy which is 1mg epinephrine 1:10,000 every 3-5 minutes rapid IV or IO push.
Do you give atropine for asystole?
Atropine is inexpensive, easy to administer, and has few side effects and therefore can be considered for asystole or PEA. The recommended dose of atropine for cardiac arrest is 1 mg IV, which can be repeated every 3 to 5 minutes (maximum total of 3 doses or 3 mg) if asystole persists (Class Indeterminate).
Do you defibrillate in asystole?
Asystole is a non-shockable rhythm. Therefore, if asystole is noted on the cardiac monitor, no attempt at defibrillation should be made. In many hospitals, it is mandatory for all healthcare workers who look after patients to be certified in BLS and ACLS.
Do you stop CPR in asystole?
Although organizations such as the American Heart Association publish and disseminate guidelines on how to perform CPR, there are few recommendations on when to stop it. Asystole — the lack of a heart rhythm — for 20 minutes is considered lethal.
Do you give adrenaline for asystole?
Adrenaline (epinephrine) is the first line drug for asystole. Through α-adrenergic−mediated vasoconstriction, its action is to increase aortic diastolic pressure during chest compressions and thus coronary perfusion pressure and the delivery of oxygenated blood to the heart.
Why do you not defibrillate asystole?
Asystole isn't a shockable rhythm, and defibrillation may actually make it harder to restart the heart. Defibrillation is only an option if your heart goes from asystole to a shockable rhythm, which is possible when someone with asystole receives effective CPR.
Do we shock asystole?
The Advanced Life Support guidelines do not recommend defibrillation in asystole. They consider shocks to confer no benefit, and go further claiming that they can cause cardiac damage; something not really founder in the evidence.
How do you reverse asystole?
Can You Reverse Asystole?Cardiopulmonary resuscitation (CPR). High-quality CPR acts like a heartbeat. This can keep blood flowing through your body.Epinephrine. Also called adrenaline, this drug can boost blood flow. Some experts think more research is needed on its role in cardiac arrest.
Do you shock asystole?
The Advanced Life Support guidelines do not recommend defibrillation in asystole. They consider shocks to confer no benefit, and go further claiming that they can cause cardiac damage; something not really founder in the evidence.
How do you reset the heart in asystole?
Can You Reverse Asystole?Cardiopulmonary resuscitation (CPR). High-quality CPR acts like a heartbeat. This can keep blood flowing through your body.Epinephrine. Also called adrenaline, this drug can boost blood flow. Some experts think more research is needed on its role in cardiac arrest.
Do you give adrenaline for asystole?
Adrenaline (epinephrine) is the first line drug for asystole. Through α-adrenergic−mediated vasoconstriction, its action is to increase aortic diastolic pressure during chest compressions and thus coronary perfusion pressure and the delivery of oxygenated blood to the heart.
How long of a pause is asystole?
Absence of escape rhythm results in asystole. Sinus pause less than 3 seconds usually needs no investigation and may be seen in normal people; however, longer pauses (≥3 seconds) require further investigation and treatment.
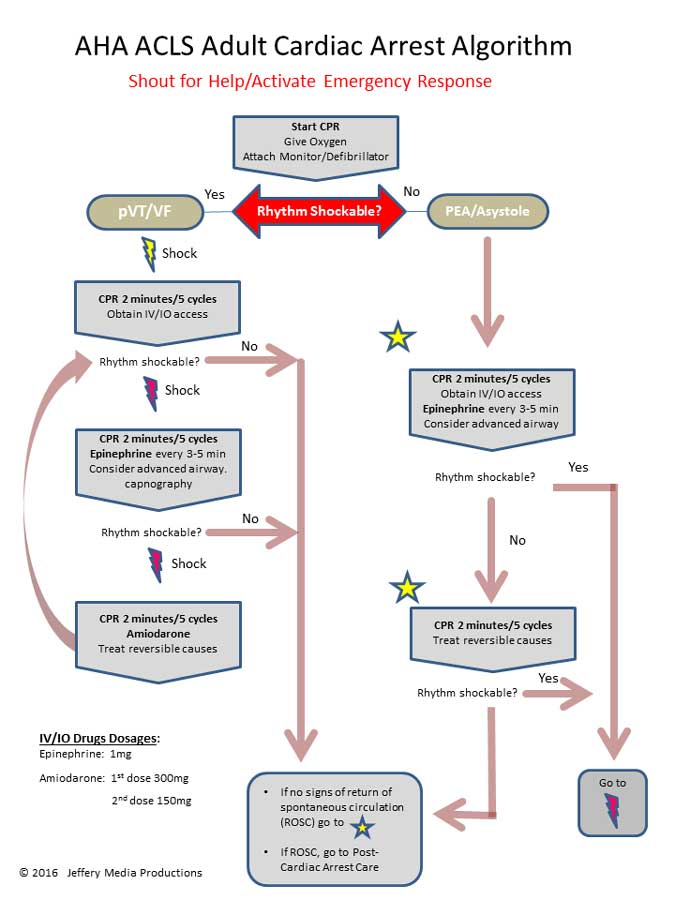
Which branch of the cardiac arrest algorithm is used for asystole?
Asystole is treated using the right branch of the Cardiac Arrest Algorithm. Click below to view the Cardiac Arrest Algorithm diagram. When done click again to close the diagram.
What is the definition of asystole?
Asystole is defined as a cardiac arrest rhythm in which there is no discernible electrical activity on the ECG monitor. Consequently, it is sometimes referred to as a “flat line.” Confirmation that a “flat line” is truly asystole is an important step in the ACLS protocol.
What is the name of the medication that produces vasoconstriction and a rise in blood pressure?
Vasopressors. A vasopressor is a medication that produces vasoconstriction and a rise in blood pressure. The vasopressor that is used for the treatment within the right branch of the Cardiac Arrest Algorithm is epinephrine. Epinephrine is primarily used for its vasoconstrictive effects.
Why should the H and T of ACLS be reviewed?
The H’s and T’s of ACLS should be reviewed to identify any underlying cause that could have precipitated the asystole.
Is asystole a good outcome?
Asystole for many patients is the result of a prolonged illness or cardiac arrest, and prognosis is very poor. Few patients will likely have a positive outcome and successful treatment of cardiac arrest with asystole will usually involve the identification and correction of an underlying cause of the asystole.
What is the best medicine for asystole?
For asystole, the standard medication to use is epinephrine.
What is an asystole?
Asystole, otherwise known as a flatline, is a state of cardiac standstill in which all electrical activity has ceased.
How often should you do a rhythm check for CPR?
Following the initial dose, epinephrine is given every 3-5 minutes as needed. During CPR, a rhythm check should be done every 2 minutes (5 cycles). These rhythm checks should be kept to less than 10 seconds, in order to prevent meaningful interruptions in CPR.
What does it mean when you have apparent asystole?
Apparent asystole may be the result of a user or technical error. If you believe the rhythm may be incorrect, ensure patches have good contact with the individual, leads are connected, the gain is set appropriately, and the power is on.
Is defibrillation effective for asystole?
Because asystole is not a shockable rhythm, defibrillation is not an effective asystole treatment. Researchers estimate that less than two percent of people who suffer asystole outside of the hospital will survive - even with trained emergency intervention.
Is asystole a flatline?
Identifying Asystole. Confirmation that the rhythm is indeed a flatline, and not a false positive, is an important part of the asystole treatment algorithm. For most patients, true asystole is the result of a prolonged illness or cardiac arrest, and prognosis is very poor.