PEG Tube Feeding - Checking Residual. That means that in 2.5 hours, nothing has left the stomach. This could be a sign that the patient is having problems with GI motility. My first action would be to return the residual, stop the tube feed and assess the patient.
How much residual is normal for PEG tube?
Thereof, how much residual is OK for tube feeding? If using a PEG tube, measure residual every 4 hours (if residual is more than 200 ml or other specifically ordered amount, hold for one hour and recheck; if it still remains high notify doctor). If using a PEG tube, reinstall residual.
How much residual tube feeding is normal?
There are no set rules in place, as feeding rates can vary greatly as well. In adults that are getting 75 ml plus an hour, it is not uncommon to see residuals at times of 150 t0 200 mls. That would be little more than two hours worth of feeds and if checking every four hous, this is quite acceptable.
Do you check residuals on peg?
In a PEG tube, we re no longer supposed to check residuals. We are supposed to check residuals in NG-tubes, but only stop the tube feeding if residuals exceed 200 mL. We immediately stop the tube feeding, check the blood sugar, call rapid response, and start suctioning her orally and doing deep NT suctioning.
How to check peg residual?
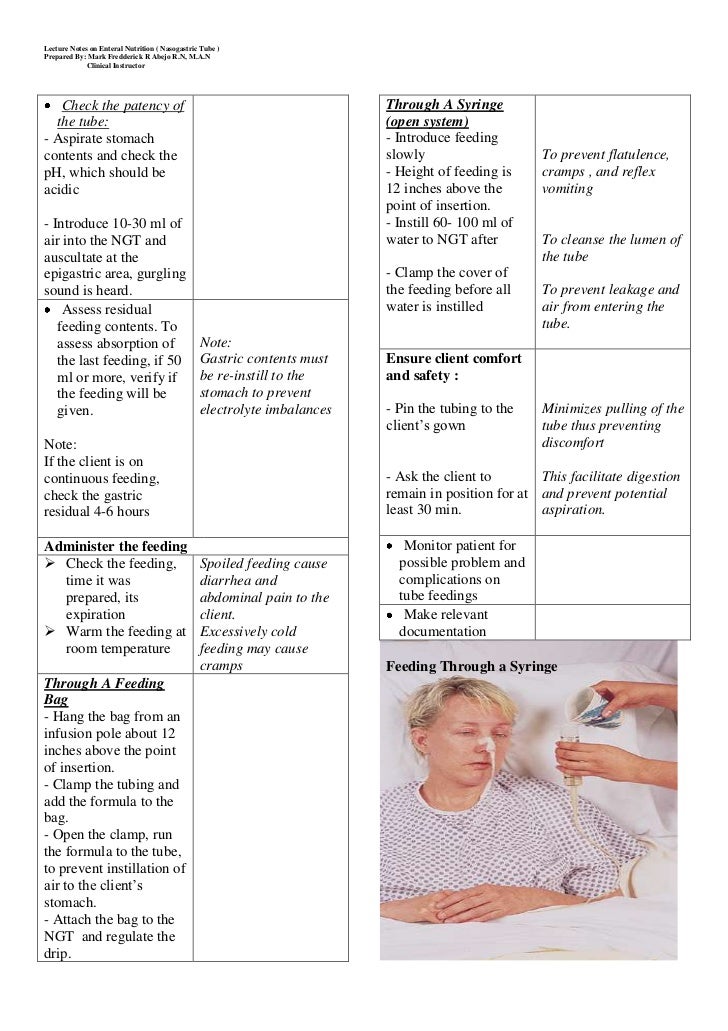
Make a residual check:
- Please wash your hands.
- Connect the feeding tube to a 60cc catheter tip syringe.
- To extract stomach contents or residuals, pull back on the syringe’s plunger.
- Allow more than 150cc of stomach content to flow back into the stomach by gravity if you draw out more than 150cc.
- Keep the feeding going for another two hours.
What does high residual mean in tube feeding?
Therefore, physical exam is equally important when assessing tube feeding tolerance. Residual refers to the amount of fluid/contents that are in the stomach. Excess residual volume may indicate an obstruction or some other problem that must be corrected before tube feeding can be continued.
What is normal residual for tube feeding?
Typically, standard nursing practice is to stop tube feedings due to gastric residual volume (GRV) that is twice the flow rate. So, a feeding rate of only 40 mL per hour would be held with a measured GRV of 80 mL.
How do you check residual on a PEG tube?
0:471:36Home Tube Feeding - Checking Residuals - YouTubeYouTubeStart of suggested clipEnd of suggested clipThe end of the syringe to your feeding tube and gently pull back on the plunger to withdraw theMoreThe end of the syringe to your feeding tube and gently pull back on the plunger to withdraw the stomach contents. Check the amount in the syringe.
Why is it important to check residual of feeding tube?
The main purpose of monitoring GRV is to improve safety in patients receiving EN. The administration of more enteral nutrients via the feeding tube while the stomach is already full (a high GRV) is not advisable in patients with reduced GI tolerance.
Do you discard gastric residual?
It's well-known that discarding the residual gastric aspirates can increase the risk of reducing energy intake, however, the very abnornal looking aspirates such as bloody, fecal or very bilious aspirates are virtually always discarded since it's a sign of gastric bleeding or intolerance [30].
What color is gastric residual?
Gastric aspirates were most frequently cloudy and green, tan or off-white, or bloody or brown. Intestinal fluids were primarily clear and yellow to bile-colored. In the absence of blood, pleural fluid was usually pale yellow and serous, and tracheobronchial secretions were usually tan or off-white mucus.
How much is too much gastric residual?
However, the extent to which bedside assessment of GRVs can help predict aspiration risk has been questioned,8 as has the amount of GRV that signals increased risk of aspiration. Values as low as 50 mL and higher than 500 mL have been reported.
What is considered high gastric residual volume?
In a review article, “Measurement of Gastric Residual Volume: State of the Science,” published in 2000 in MEDSURG Nursing, Edwards and Metheny reported that the literature contained a variety of recommendations for what is considered a high GRV, ranging from 100 to 500 mL.
Why do we check residuals?
In most hospitals, gastric residuals are monitored for all patients who receive enteral feeding. The theory is that patients with larger residuals will be at greater risk for vomiting, subsequent aspiration, and ventilator-associated pneumonia (VAP).
Should you check residuals?
Based on this, experts initially suggested checking residuals, typically every 4-6 hours, for the large quantities of feed and gastric content. However, no studies have shown that increased gastric volume increases VAP risk, ICU-acquired infections, or aspiration.
What is considered high gastric residual volume?
In a review article, “Measurement of Gastric Residual Volume: State of the Science,” published in 2000 in MEDSURG Nursing, Edwards and Metheny reported that the literature contained a variety of recommendations for what is considered a high GRV, ranging from 100 to 500 mL.
How much residuals is too much?
Tube feeding intolerance has a wide definition, but most commonly is defined as high gastric residual, increased abdominal size/distention, discomfort or emesis. There is a wide range in what was considered as high residual, anywhere from 100-500 cc, showing no clear consensus on what number to use.
What is normal nasogastric tube output?
The average daily nasogastric output was 440 +/- 283 mL (range 68-1565).
How long should head of bed be elevated after tube feeding?
If unable to sit up for a bolus feed or if receiving continuous feeding, the head of the bed should be elevated 30-45 degrees during feeding and for at least 30 minutes after the feed to reduce the risk of aspiration.
Why do you not check residual on PEG tube?
A: I do not have the ability to check residual on PEG tube.
Can you check gastric residual in gastrostomy tube?
A: Gastric residual is the amount of food in the stomach after a meal has been digested. It can be measured using different devices, or with an abo...
Can you aspirate with a PEG tube?
A: Nowadays it is more common to use PEG tubes rather than tracheotomy tubes. This is due to the fact that they are easier on soft tissues and do n...
How often should you check residuals?
with a continuous feeding, check the residuals every 4 hours and before any flush or medication administration.
Do we check residuals on continuous feeds?
on our floor, we check residuals with our scheduled flushes for pts on continuous feeds . i'd check residuals more frequently on pts who have distended abd, who havent had a bm for a while.
Why does a Pt have residuals?
One of the reasons a pt has residuals is because the stomach doesn't exactly empty at a continuous rate. The stomach is a mixing chamber...nothing more. Tube feedings need little digestion and it should pass relatively quick, but the stomach is at the mercy of the pyloric sphincter and the vagus nerve.
How to get a PT to empty?
There is on quick thing you can do from a nursing stand point. Put the pt on their right side. The pylorus is down and to the right. If the pt is completely on their left side, there is delayed emptying. What doesn't pass by peristalsis will stay in the stomach and build. Residuals don't count unless you've mobilized the pt a bit and put them on the right side. Give them a chance to empty. When they are on the right side, all the tube feeding (which has been pooling in the greater curvature of the stomach) will pool above the pylorus, causing stretch and emptying. You basically stimulate the parasympathetic response by manipulating the feedings. If that doesn't work, then they aren't tolerating.
What is the activity of the pylorus?
So here it the kicker.....the activity of the pylorus is related to the stretching of the stomach wall (among other things). Some people need a certain amount of food in the stomach before the pylorus can expand larger enough to pass feedings. So it goes build, build, build, empty...build, build, build, empty.
Is the pylorus closed off?
Now, the pylorus isn't completely closed off and tube feedings can pass very quickly (because there's really nothing to digest) but, in some pts, the pylorus may only be open enough for a few drops to pass a second. And that may be enough to build over time.
What is a PEG tube?
A percutaneous endoscopic gastrostomy (PEG) is a surgery to place a feeding tube. Feeding tubes, or PEG tubes, allow you to receive nutrition through your stomach. You may need a PEG tube if you have difficulty swallowing or can't get all the nutrition you need by mouth.
What is the procedure to place a PEG tube?
Most healthcare providers place PEG tubes with endoscopic surgery. Endoscopic procedures use small incisions and a long, flexible instrument called an endoscope. On the day of surgery, you receive intravenous (IV) anesthesia and antibiotics. The anesthesia ensures that you remain calm and numb during the procedure.
Why do people need peg tubes?
People who need PEG tubes because of swallowing problems have restrictions on eating and drinking by mouth. Some people may still eat and drink small amounts through the mouth.
What is the tube called that feeds the stomach?
These feeding tubes are often called PEG tubes or G tubes. The tube allows you to receive nutrition directly through your stomach. This type of feeding is also known as enteral feeding or enteral nutrition.
What are the risks of percutaneous endoscopic gastrostomy?
Possible risks of percutaneous endoscopic gastrostomy include: Accidental tube dislodgement (tube moving out of place or coming out). Aspiration (accidentally inhaling your stomach contents). Bleeding and perforation (hole in the wall of your bowel or intestine). Infection near the incision. Pain near the PEG tube.
How long does it take for a peg tube to heal?
Usually, your surgeon will give you instructions to remove the bandage after one to two days. After the area around your feeding tube heals, you’ll meet with a dietitian. This specialist explains how to use the PEG tube and starts you on enteral nutrition.
Why do we need feeding tubes?
Feeding tubes may also be useful if you have a condition that interferes with how your body processes nutrition. For example, you may benefit from a PEG tube if you have cystic fibrosis or receive dialysis for kidney failure. Someone in a coma may receive a PEG tube to help keep them alive.