The subacromial space lies below the coracoacromial arch and above the humeral head and greater tuberosity of the humerus. The coracoacromial arch consists (lateral to medial) of the acromion, the coracoacromial ligament (anterior to the acromioclavicular joint), and coracoid process.
Full Answer
What causes the coracoacromial arch to flare up?
Overuse of the shoulder: Repetitive microtrauma can result in soft tissue inflammation of the rotator cuff tendons and the subacromial bursa, leading to friction between the tendons and the coracoacromial arch
What is the coracoacromial arch made of?
The coracoacromial arch is formed by the acromion, coracoacromial ligament, and the tip of the coracoid process. tuberosity. Compromise of the space within the coracoacromial arch results in “outlet impingement.” FIGURE 3-2. Rotator cuff. A: Posterior view. B: Anterior view. The rotator cuff consists of the supraspinatus,
Where is the coracoacromial ligament located?
The left shoulder and acromioclavicular joints, and the proper ligaments of the scapula. (Coraco-acromial visible at upper right.) Glenoid fossa of right side. The coracoacromial ligament is a strong triangular ligament between the coracoid process and the acromion.
What is the subacromial space in the human body?
The Subacromial Space The subacromial space lies below the coracoacromial arch and above the humeral head and greater tuberosity of the humerus. The coracoacromial arch consists (lateral to medial) of the acromion, the coracoacromial ligament (anterior to the acromioclavicular joint), and coracoid process.
What muscle passes under the coracoacromial Arch?
The supraspinatus (Fig. 2.24) arising from the supraspinous fossa of scapula is related to the superior aspect of shoulder. The tendon of the muscle passes deep to the coracoacromial ligament to gain insertion to the greater tubercle and the superior aspect of the capsule of the shoulder joint.
What is the role of the coracoacromial Arch?
Together with the inferior aspect of the acromion and the coracoid process of the scapula, the CAL forms the coracoacromial arch that acts to limit superior displacement of the humeral head from the glenoid (Figure 1).
What are the components of coracoacromial Arch?
The coracoacromial arch consists of the acromion, coracoacromial ligament, and coracoid process. If the coracoacromial arch is violated, these patients may also demonstrate superior escape of the humeral head.
Is the coracoacromial arch a ligament?
Coracoacromial arch is a term for different bony and ligamentous structures, which form the superior border supraspinatus outlet 1-4.
What motion does the coracoacromial ligament restrict?
Contracture of the coracohumeral ligament is reported to restrict external rotation of the shoulder with arm at the side and restrict posterior-inferior shift of the humeral head. The contracture is supposed to restrict range of motion of the glenohumeral joint.
Where does the coracoacromial ligament run?
Structure. The coracoacromial ligament originates from the summit of the acromion of the scapula, just in front of the articular surface for the clavicle. It inserts by its broad base along the whole length of the lateral border of the coracoid process of the scapula.
Where is the coracoacromial Arch?
the scapulaThe coracoacromial arch is the superior lateral extension of the scapula and is comprised of the acromion, coracoacromial ligament, and coracoid (Fig. 1).
What is a positive Hawkins Kennedy test?
A positive Hawkins-Kennedy test is indicative of an impingement of all structures that are located between the greater tubercle of the humerus and the coracohumeral ligament. The impinged structures include the supraspinatus muscle, teres minor muscle, and the infraspinatus muscle.
What is a CA ligament release?
Release of the CA ligament resulted in increased anterior and inferior translation of the internally and externally rotated glenohumeral joint. The CA ligament has previously been implicated only as an important soft tissue structure that contributes to rotator cuff pain.
What ligament along with the acromion forms the coracoacromial arch quizlet?
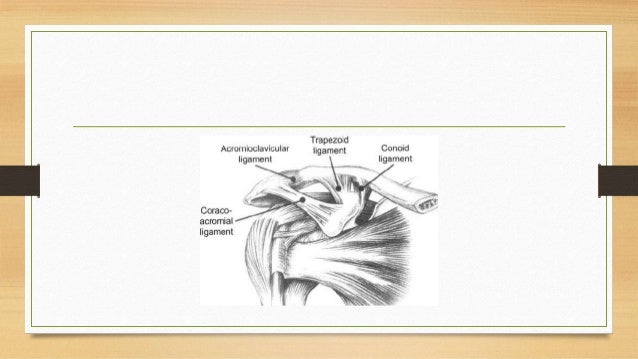
The acromioclavicular ligament along with the coracoclavicular ligament helps to maintain the position of the clavicle relative to the acromion. The coracoacromial ligament connects the coracoid to the acromion. This ligament along with the acromion forms the coracoacromial arch.
What does the coracoclavicular ligament do?
The coracoclavicular ligament, as described above, serves to connect the clavicle and the coracoid process of the scapula. Its two-component structure allows for proper apposition of the acromion and the clavicle while preventing vertical displacement of the scapula with respect to the clavicle.
What is a positive Hawkins Kennedy test?
A positive Hawkins-Kennedy test is indicative of an impingement of all structures that are located between the greater tubercle of the humerus and the coracohumeral ligament. The impinged structures include the supraspinatus muscle, teres minor muscle, and the infraspinatus muscle.
What ligament along with the acromion forms the coracoacromial arch quizlet?
The acromioclavicular ligament along with the coracoclavicular ligament helps to maintain the position of the clavicle relative to the acromion. The coracoacromial ligament connects the coracoid to the acromion. This ligament along with the acromion forms the coracoacromial arch.
Which part of the shoulder joint capsule is weakest?
The weakest area of the shoulder joint capsule is just anterior to the attachment of the long head of the triceps at the infraglenoid tubercle, and disloca- tions are most frequent in this inferior anterior region.
Which tendons make up the rotator cuff?
The rotator cuff consists of four muscles. These are the subscapularis, the supraspinatus, the infraspinatus and the teres minor muscles. These muscles end in short, flat, broad tendons which fuse intimately with the fibrous capsule to form the musculotendinous cuff.
What causes acromial subluxation?
Glenohumeral instability: Any abnormality of the glenohumeral joint or weakness in the rotator cuff muscles can lead to superior subluxation of the humerus, causing an increased contact between the acromion and subacromial tissues
Where is the subacromial space?
The Subacromial Space. The subacromial space lies below the coracoacromial arch and above the humeral head and greater tuberosity of the humerus. The coracoacromial arch consists (lateral to medial) of the acromion, the coracoacromial ligament (anterior to the acromioclavicular joint), and coracoid process.
What is the subacromial bursa?
Within the subacromal space run the rotator cuff tendons, the long head of biceps tendon, and the coraco-acromial ligament, all surrounded by the subacromial bursa which helps to reduce friction between these structures.
What causes the humerus to move proximally?
Intrinsic mechanisms involve pathologies of the rotator cuff tendons due to tension, including: Muscular weakness: Weakness in the rotator cuff muscles can lead to muscular imbalances resulting in the humerus shifting proximally towards the body.
Is decompression better than arthroscopy?
However, recent evidence from a randomised surgical trial showed that surgical decompression appeared to offer no extra benefit over arthroscopy alone, and indeed that the benefits seen from the surgical intervention might only be the result of a placebo effect or the increased post-operative physiotherapy.
What is the subacromial space?
The subacromial space lies directly inferior to the acromion, the coracoid process, the acromioclavicular joint, and the coracoacromial ligament (see Figure 30-1). Lubricated by the subacromial bursa, the subacromial space in health is narrow and the anatomical structures surrounding it are responsible for maintaining static and dynamic shoulder stability. The space between the acromion and the superior aspect of the humeral head is the impingement interval, and abduction of the arm narrows the space further (see Figure 30-2 ). Any pathological condition that further narrows this space (e.g., osteophyte, abnormal acromial anatomy, ligamentous calcification, or congenital defects of the acromion) increases the incidence of impingement (see Figure 30-3 and Table 30-1Figure 30-3Table 30-1 ).
Which joint is compressed by crossing the arm horizontally?
By crossing the arm horizontally maximally across the chest ( Fig. 57.8 ), compression of the ipsilateral acromioclavicular joint occurs.
What type of acromion is associated with spinal impingement syndrome?
These include type 2 and type 3 acromions ( Figure 30-4 ). Although the “normal” type 1 acromion is relatively flat, the type 2 acromion curves downward and the type 3 acromion hooks downward in the shape of a scimitar. The downward curve of the type 2 and type 3 acromions markedly narrow the subacromial space ( Figure 30-5 ). In addition to these anatomical variations, a congenitally unfused acromial apophysis, the os acromiale, is often associated with subacromial impingement syndrome ( Figure 30-6 ).
How to perform hemiarthroplasty?
The patient is placed in the beach-chair position with the head of the bed at 35–45° and all bo ny prominences are padded. An interscalene block is placed preoperatively, and general anesthesia is administered. The arm is positioned such that AP and axillary radiographs may be obtained. A deltopectoral approach is utilized from 2 to 3 cm proximal to the coracoid to a point at or near the deltoid tuberosity. The cephalic vein is encountered and frequently taken laterally with the deltoid. The deltoid and pectoralis major are retracted utilizing Richardson retractors. The clavipectoral fascia is incised just lateral to the coracobrachialis, and this incision is taken superiorly to the coracoacromial (CA) ligament. At this time, the fracture hematoma can be visualized and removed. The anterior edge of the CA ligament is excised and removed improving superior exposure, which allows for improved access to the tuberosities for suture placement. The biceps tendon is encountered just proximal to the medial and superior edge of the pectoralis major tendon. The tendon is traced upward into the joint, exposing the bicipital groove.
How to detect supraspinatus atrophy?
The clinician detects atrophy of the supraspinatus or infraspinatus muscles by inspecting the posterior scapula on the symptomatic side and noting any increased prominence of the scapular spine when compared with the contralateral side. Atrophy of these muscles may appear as soon as 2 to 3 weeks after a rotator cuff tear.
What is the procedure to transfer the CA ligament?
Coracoacromial (CA) ligament transfer (Weaver–Dunn) and its modifications consist of detaching the CA ligament from the acromion and transferring the free ends to the distal end of the clavicle through drill holes ( Hedtmann et al., 1998 ). Some historical success has been attributed to this procedure, although failure rates (clinical and radiographic) are fairly high, ranging from 14% to 50% depending on the study ( Sood et al., 2008; Rauschning et al., 1980) and whether the Weaver–Dunn procedure was performed for an acute or chronic injury ( Warren-Smith and Ward, 1987 ). Loss of reduction occurs again due to the high forces sustained by the AC joint ( Tauber et al., 2007; LaPrade and Hilger, 2005) and failure occurs via stretching of the transferred ligament.
Where are tuberosities placed before suturing?
Sutures are placed horizontally at the tendon bone junction of the infraspinatus, teres minor across to the subscapularis, and tied for a horizontal repair. An “around the world” stitch has been popularized to secure the fixated tuberosities to the prosthesis as well ( Frankle et al., 2002 ).
What are the soft tissues that pass under the coracoacromial arch?
Soft tissues such as the supraspinatus tendon, subacromial bursa, joint capsule, coracohumeral ligament, and biceps brachii tendon all pass underneath the coracoacromial arch (Fig. 1). During shoulder flexion or abduction, any of these soft tissues can be compressed under the coracoacromial arch; repeated compression can cause fraying, irritation and inflammation. Compression of the soft tissues underneath the coracoacromial arch is referred to as shoulder impingement syndrome.
What is the subacromial region?
The subacromial region lies beneath the coracoacromial arch. This arch is formed by two bony projections, the coracoid process and acromion process of the scapula. The coracoacromial ligament spans between these two bony prominences to form the arch.
What causes a scapula to not fully rotate?
When the scapula doesn’t fully rotate upward during abduction, the greater tubercle of the humerus pinches soft tissues against the underside of the acromion (shoulder impingement). This pattern reminds us that it is important to look at a variety of factors that can contribute to shoulder impingement; sometimes the cause may be a bit more elusive than is immediately apparent.
What is the movement of the shoulder called?
This coordinated movement is referred to as the scapulothoracic rhythm. Various conditions, such as adhesive capsulitis ( frozen shoulder ), cause a significant alteration of the scapulohumeral rhythm.
What are the two main bones of the shoulder complex?
Any discussion of shoulder pathologies must start with a solid understanding of the anatomical and biomechanical challenges in this area. The scapula and humerus are the two main bones of the shoulder complex, although the clavicle is another essential bone in the shoulder girdle.
What is the pain in the anterior shoulder?
Pain on the anterior aspect of the shoulder is more likely the result of a distal subscapularis or biceps tendon disorder. Using appropriate assessment strategies helps you narrow down the focus for your treatments so they can have the greatest success.
What is shoulder abduction?
For example, shoulder abduction involves coordinated movement between the scapula and humerus. Full abduction requires upward rotation of the scapula along with glenohumeral abduction in a specific ratio.
How is subacromial decompression performed?
A subacromial decompression is usually performed arthroscopically i.e. keyhole surgery using the following procedure: A tube is inserted into the first hole through which fluid is pumped to expand the shoulder joint so that the surgeon can see better and have better access to the acromion.
What is subacromial decompression?
A subacromial decompression aka acromioplasty is an operation performed to treat shoulder impingement. Impingement occurs when soft tissues in the shoulder repeatedly rub against bone causing pain and inflammation, particularly when you raise your arm. The aim of shoulder impingement surgery is to regain full, pain-free range ...
How long does subacromial decompression surgery take?
Subacromial decompression surgery typically takes less than an hour and in most cases, you will be allowed home the same day – you will need someone to drive you home.
What is the area of the shoulder called?
At the top of the shoulder, part of the shoulder blade, known as the acromion, and one of the ligaments, the coracoacromial ligament, join together to form a sort of arch/roof. Underneath this arch is an area known as the subacromial space, through which the rotator cuff tendons pass. As the arm lifts up, the subacromial space narrows.
What is the purpose of the third hole in the subacromial decompression?
Specially designed surgical instruments are inserted through the third hole to remove any problem areas of bone and soft tissues that are found. Depending on the cause of the impingement, subacromial decompression may involve some or all of the following:
How long does it take to get relief from subacromial decompression?
If you wait until you have pain to take your painkillers, it is harder to manage the pain as medication can take up to an hour to relieve symptoms. Around three days after your subacromial decompression, you should be able to start reducing the level of medication - your doctor will advise you on what medications to take and how often.
When is subacromial decompression surgery recommended?
Subacromial decompression surgery is recommended if non-operative treatment , such as exercises and injections have failed or if significant bone spurs have developed on the acromion.
How high is the acromion?
acromion. Elevation is generally limited to 30 or 40 degrees. This is a
What is tuberosity in arch?
tuberosity. Compromise of the space within the coracoacromial arch
Which component includes the infraspinatus tendon?
avulsion component that includes the infraspinatus tendon. As rotator
