A patient with severe ischemic or hemorrhagic stroke needs to have a tracheostomy performed if he remains unable to breathe and protect his airway sufficiently.
When do you need a tracheostomy after a stroke?
There, tracheostomy will be chosen if extubation fails or is deemed not feasible, that is, as part of weaning from the ventilator. The need of tracheostomy, the timing of tracheostomy, and its potential benefits versus risks to the patient with severe stroke remain challenging and controversial.
Why would I need a tracheostomy?
You can change your cookie settings at any time using our cookies page. A tracheostomy is sometimes needed if you're unable to breathe normally because of an underlying health condition or a blocked airway. A tracheostomy can deliver oxygen to the lungs if you cannot breathe normally.
What are the risks of a tracheostomy?
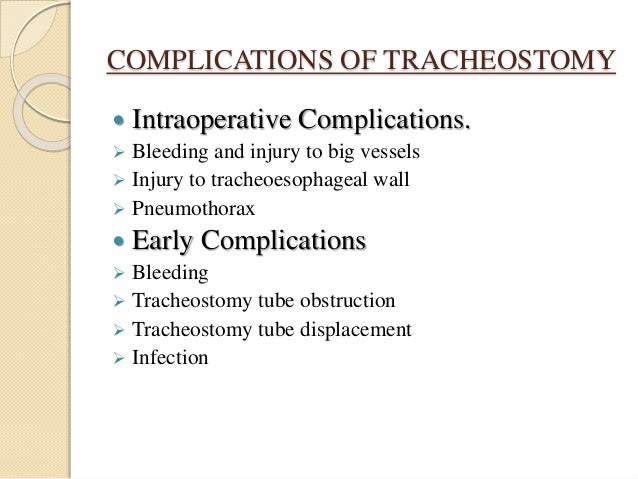
Risks. 1 Bleeding at the tracheostomy site or from the trachea. 2 Difficulty breathing through the tube. 3 Pain or a change in comfort level. 4 Redness or swelling around the tracheostomy. 5 A change in the position of your tracheostomy tube.

Is it normal to be on a ventilator after a stroke?
Background and purpose: Intubation and mechanical ventilation are sometimes necessary during treatment of acute stroke. Indications include neurological deterioration, pulmonary complications, and elective intubation for procedures and surgery.
What are the signs of death after a stroke?
found a high prevalence of certain symptoms among dying stroke patients (n = 42), namely, dyspnea (81%) and pain (69%), mouth dryness (62%), and anxiety (26%)[12].
How does stroke cause respiratory failure?
Stroke may disrupt breathing either by (A) causing a disturbance of central rhythm generation, (B) interrupting the descending respiratory pathways leading to a reduced respiratory drive, or (C) causing bulbar weakness leading to aspiration.
Why would you do a tracheostomy instead of intubation?
Tracheostomy is thought to provide several advantages over translaryngeal intubation in patients undergoing PMV, such as the promotion of oral hygiene and pulmonary toilet, improved patient comfort, decreased airway resistance, accelerated weaning from mechanical ventilation (MV) [4], the ability to transfer ventilator ...
What is the most critical time after a stroke?
The results strongly suggest that there is a critical time window for rehabilitation following a stroke. For this study, that window was 2-3 months after stroke onset. Larger clinical trials are needed to better pin down the timing and duration of this critical window.
What is the most serious type of stroke?
Doctors discovered she was having a hemorrhagic stroke. Most strokes are caused by a clot that cuts off blood flow to the brain. But about 13 percent are caused by a weakened blood vessel that ruptures and bleeds into the brain. These so-called hemorrhagic strokes are the deadliest and least treatable type.
Can you regain swallowing after stroke?
Over half of stroke survivors experience dysphagia after their stroke event. Thankfully, the majority of survivors “recover swallowing function within 7 days, and only 11-13% remain dysphagic after six months.”
What type of stroke affects breathing?
A stroke that happens in the brain stem, where your body's vital functions — like breathing, heartbeat, and body temperature — are controlled can also cause breathing problems. This type of stroke is more likely to result in coma or death.
What happens to the respiratory system after a stroke?
Stroke can lead to sleep disordered breathing such as central or obstructive sleep apnea. Sleep disordered breathing may also play a role in the pathogenesis of cerebral infarction. Venous thromboembolism, swallowing abnormalities, aspiration, and pneumonia are among the most common respiratory complications of stroke.
Is a trach considered life support?
A healthy person clears mucus by swallowing or coughing. For people with a tracheostomy — a breathing tube in their throat — the mucus gets trapped in their lungs. It has to be suctioned several times throughout the day. The procedure is life-saving.
What is the life expectancy of a person with a tracheostomy?
The median survival after tracheostomy was 21 months (range, 0-155 months). The survival rate was 65% by 1 year and 45% by 2 years after tracheostomy. Survival was significantly shorter in patients older than 60 years at tracheostomy, with a hazard ratio of dying of 2.1 (95% confidence interval, 1.1-3.9).
How serious is a tracheostomy?
A tracheostomy is generally a safe procedure that works well. However, as with all medical procedures, there's a small risk of complications, including: bleeding. damage to the tube that carries food from the throat to the stomach (oesophagus)
What is the prognosis for stroke patients that require mechanical ventilation?
INTRODUCTION: The prognosis for stroke patients that requiring mechanical ventilation is poor with mortality rates up to 80%. Airway management in ischemic stroke patients is of great significance for achieving a better clinical outcome. After endotracheal intubation, tracheostomy is recommended if patients require long-term ventilation. In this study, it is aimed to present the outcomes of percutaneous and surgical tracheostomy in ischemic stroke patients that were monitored in Neurological Intensive Care Unit (NICU). METHODS: Patients with ischemic stroke admitted to NICU and underwent tracheostomy were reviewed retrospectively. Age, sex, mechanical ventilation time prior to tracheostomy, timing of tracheostomy, complications related to tracheostomy and mortality/discharge state were recorded. Patients were categorized into two groups as percutaneous tracheostomy or surgical tracheostomy groups. RESULTS: This study presents 76 patients with ischemic stroke that underwent tracheostomy procedure in NICU. Thirty-nine patients were in percutaneous tracheostomy (PT) group and 37 patients were in surgical tracheostomy (ST) group. There was no significant difference between the two groups regarding tracheostomy complications and mortality rates. DISCUSSION AND CONCLUSION: Based on our seven years of clinical experience, we conclude that PT can be performed at bedside in a short time and is associated with low complication rates. PT can be conveniently applied to indicate patients by neurologists (working in NICU) after proper training.
How does stroke affect the UK?
Stroke is a leading cause of death and adult disability in the UK. A stroke can have significant negative effects on the lives of patients and their families and carers. While improved stroke management has contributed to a reduction in mortality and improved outcomes following rehabilitation, the incidence of stroke continues to rise in the UK, partly because of the ageing population. Stroke rehabilitation involves a multidisciplinary approach, with nurses performing a central role. This article describes the risk factors and types of stroke, the main areas of stroke rehabilitation and the role of the nurse. It emphasises that providing support to families and carers is a particularly important element of caring for people who have experienced a stroke.
What is SP in stroke?
Background/aims: Substance P (SP) is a neuropeptide, likely acting as a neurotransmitter in the pharyngeal mucosa enhancing the swallow and cough reflex. Pharyngeal Electrical Stimulation (PES) induces a temporary increase of salivary SP levels in healthy adults. Previous evidence suggests that post-stroke dysphagia is related to reduced SP levels. Here, we investigated the effects of PES on SP levels in severely dysphagic stroke patients and a possible link between increase of SP and treatment success. Methods: 23 tracheotomized stroke patients who could not be decannulated due to severe and persisting dysphagia according to endoscopic evaluation received PES for 10 minutes a day over three consecutive days in this prospective single-center study. If initial treatment failed, repetitive stimulation cycles were provided. Saliva samples were collected before and directly after each PES. Results: 61% of participants were decannulated after the first treatment cycle. Increase of SP levels post-stimulation was closely related to treatment success, i.e. decannulation with 79% of successfully treated patients showing increase of SP, whereas 89% of unsuccessfully treated patients had stable or decreased SP levels. Applying logistic regression analysis, increase of SP level remained the only independent predictor of decannulation after PES. All 3 repetitively treated patients showed increased SP levels when progressing from the 1st to the 2nd cycle, two of whom were decannulated hereafter. Conclusions: The physiological mechanism of PES may consist in restoration of sensory feedback, which is known to be crucial for the execution of a safe swallow. SP possibly acts as a biomarker for indicating response to PES.
What is neurocritical care?
Neurocritical care is an ever-evolving discipline and its implementation in intensive care leads to reduction in mortality and to improvement of functional outcome in patients with devastating injuries to the nervous system. However, the decisive elements of the complete field of neurocritical care remain relatively unclear, as well as the exact ways to optimize them. During recent years new insights have been gained and new exciting studies have been initiated from which results are soon to be expected. This review focuses on the following management aspects: neuromonitoring, airway and ventilation, endovascular therapy, cerebrospinal fluid drainage, decompressive craniectomy, hematoma evacuation, blood pressure, and targeted temperature management. The application of these measures to brain diseases and injuries frequently treated in neurointensive care units will be addressed in the context of current studies.
What causes acute respiratory failure?
Many neurological diseases may cause acute respiratory failure (ARF) due to involvement of bulbar respiratory center, spinal cord, motoneurons, peripheral nerves, neuromuscular junction, or skeletal muscles. In this context, respiratory emergencies are often a challenge at home, in a neurology ward, or even in an intensive care unit, influencing morbidity and mortality. More commonly, patients develop primarily ventilatory impairment causing hypercapnia. Moreover, inadequate bulbar and expiratory muscle function may cause retained secretions, frequently complicated by pneumonia, atelectasis, and, ultimately, hypoxemic ARF. On the basis of the clinical onset, two main categories of ARF can be identified: (i) acute exacerbation of chronic respiratory failure, which is common in slowly progressive neurological diseases, such as movement disorders and most neuromuscular diseases, and (ii) sudden-onset respiratory failure which may develop in rapidly progressive neurological disorders including stroke, convulsive status epilepticus, traumatic brain injury, spinal cord injury, phrenic neuropathy, myasthenia gravis, and Guillain–Barré syndrome. A tailored assistance may include manual and mechanical cough assistance, noninvasive ventilation, endotracheal intubation, invasive mechanical ventilation, or tracheotomy. This review provides practical recommendations for prevention, recognition, management, and treatment of respiratory emergencies in neurological diseases, mostly in teenagers and adults, according to type and severity of baseline disease.
Can a stroke patient have a tracheostomy?
Opinion statement: Patients with severe ischemic and hemorrhagic stroke may require tracheostomy in the course of their disease. This may apply to stroke unit patients whose deficits include a severe dysphagia posing such risk of aspiration as it cannot be sufficiently counteracted by tube feeding and swallowing therapy alone. More often, however, tracheostomy is performed in stroke patients so severely afflicted that they require intensive care unit treatment and mechanical ventilation. In these, long-term ventilation and prolonged insufficient airway protection are the main indications for tracheostomy. Accepted advantages are less pharyngeal and laryngeal lesions than with prolonged orotracheal intubation, better oral hygiene and nursing care, and higher patient comfort. Optimal timing of tracheostomy is unclear, in general, as in stroke intensive care unit patients. Potential benefits of early tracheostomy concerning ventilation duration and length of stay, respirator weaning, airway safety, rate of pneumonia, and other complications, outcome and mortality have been suggested in studies on non-neurologic subgroups of critical care patients. Stroke patients have hardly been investigated with regard to these aspects, and mainly retrospectively. A single randomized pilot trial on early tracheostomy in 60 ventilated patients with severe hemorrhagic and ischemic stroke demonstrated feasibility, safety, and less need of sedation. Regarding the technique, bedside percutaneous dilational tracheostomy should be preferred over surgical tracheostomy because of several reported advantages. As the procedural risk is low and early tracheostomy does not seem to worsen the clinical course of the ventilated stroke patient, it is reasonable to assess the need of further ventilation at the end of the first week of intensive care and proceed to tracheostomy if extubation is not feasible. Reliable prediction of prolonged ventilation need and outcome benefits of early tracheostomy, however, await further clarification. Decannulation of stroke patients after discontinued ventilation has to follow reliable confirmation of swallowing ability, as by endoscopy.
Does absorbent foam help with tracheostomy site infection?
Absorbent foam dressing may be able to prevent proliferation of infectious microorganisms by absorbing the tracheostomy stoma exudate. This study aimed to compare the efficacy of absorbent foam with gauze dressing for prevention of tracheostomy site infection. Materials and methods: In this double-blind randomized clinical trial, 80 patients (18 to 60 years) hospitalized in the intensive care unit (ICU) due to severe head injury were randomly divided into two groups and early tracheostomy was done for them during the first 2 days. In the first group, gauze was used as tracheostomy site dressing, while in the second, absorbent foam, was placed. Tracheostomy site was checked daily for any sign of infection and samples were taken from the stoma for culture in case of presence of any sign of infection. Results: Of a total of 80, 11 had tracheostomy site infection (13.75%), including 7 (17.5%) in the gauze group and 4 (10%) in the foam group. The difference in this regard between the two groups was not significant (P=0.051). Also, the dominant strains in the culture of gauze group were hospital-acquired Gram-negative bacteria (particularly Acinetobacter), while in the foam group, Gram-positives and more commonly Staphylococcus epidermidis were found. Conclusion: Absorbent foam dressing is not superior to gauze dressings for prevention of tracheostomy site infection.
What is the research about?
Some patients who have had a severe stroke can’t breathe on their own. When this happens, doctors put a breathing tube in the patient’s windpipe, and a machine pumps air into the lungs. But having a breathing tube for a long time can be uncomfortable for patients and can cause problems such as throat ulcers.
Who can this research help?
Results from this study can guide doctors, patients, and caregivers facing decisions about treatment following severe stroke and breathing failure.
What is the research team doing?
The research team is recruiting 380 patients who have had a severe stroke and are in 1 of 20 intensive care units, or ICUs, in the United States and Germany. Patients are eligible for the study if a doctor predicts that the patient will need a breathing tube and ventilation machine for two weeks or more.
Why do you need a tracheostomy?
Why it's used. A tracheostomy is sometimes needed if you're unable to breathe normally because of an underlying health condition or a blocked airway.
Why does my throat swell after tracheostomy?
A tracheostomy can also be used to bypass an airway that's blocked as a result of: accidentally swallowing something that gets stuck in the windpipe (trachea) an injury, infection, burn or severe allergic reaction (anaphylaxis) that causes the throat to become swollen and narrowed. swelling after head or neck surgery.
What causes a child's airways to narrow?
a cancerous tumour – this can sometimes happen with mouth cancer, laryngeal cancer or thyroid gland cancer. In addition, some children born with birth defects that cause their airways to be abnormally narrow may need a tracheostomy to help them breathe.
Why do we need a tracheostomy?
A tracheostomy is often needed when health problems require long-term use of a machine (ventilator) to help you breathe. In rare cases, an emergency tracheotomy is performed when the airway is suddenly blocked, ...
What happens if you have a tracheostomy after you leave the hospital?
Infection around the tracheostomy or infection in the trachea and bronchial tubes (tracheobronchitis) and lungs (pneumonia) If you still need a tracheostomy after you've left the hospital, you'll need to keep regularly scheduled appointments for monitoring possible complications.
How to get rid of tracheostomy secretions?
Putting small amounts of saline directly into the tracheostomy tube, as directed, may help loosen secretions. Or a saline nebulizer treatment may help. A device called a heat and moisture exchanger captures moisture from the air you exhale and humidifies the air you inhale.
How is a tracheostomy tube inserted?
A tracheostomy tube is inserted through the hole and secured in place with a strap around your neck. Tracheostomy (tray-key-OS-tuh-me) is a hole that surgeons make through the front of the neck and into the windpipe (trachea). A tracheostomy tube is placed into the hole to keep it open for breathing. The term for the surgical procedure ...
What is a tracheostomy tube?
Overview. A tracheostomy is a surgically created hole (stoma) in your windpipe (trachea) that provides an alternative airway for breathing. A tracheostomy tube is inserted through the hole and secured in place with a strap around your neck. Tracheostomy (tray-key-OS-tuh-me) is a hole that surgeons make through the front ...
What are the complications of a tracheostomy?
Long-term complications are more likely the longer a tracheostomy is in place. These problems include: Obstruction of the tracheostomy tube. Displacement of the tracheostomy tube from the trachea.
When is a tracheostomy performed?
In rare cases, an emergency tracheotomy is performed when the airway is suddenly blocked, such as after a traumatic injury to the face or neck. When a tracheostomy is no longer needed, it's allowed to heal shut or is surgically closed. For some people, a tracheostomy is permanent. Mayo Clinic's approach.
What conditions require a tracheostomy?
Conditions that may require a tracheostomy include: anaphylaxis. birth defects of the airway. burns of the airway from inhalation of corrosive material. cancer in the neck. chronic lung disease. coma. diaphragm dysfunction. facial burns or surgery.
How does a tracheostomy work?
A tracheostomy is a medical procedure — either temporary or permanent — that involves creating an opening in the neck in order to place a tube into a person’s windpi pe. The tube is inserted through a cut in the neck below the vocal cords. This allows air to enter the lungs.
What is the name of the hole in the neck that the tube passes through?
Breathing is then done through the tube, bypassing the mouth, nose, and throat. A tracheostomy is commonly referred to as a stoma. This is the name for the hole in the neck that the tube passes through.
What are the risks of a tracheostomy?
Risks specific to a tracheostomy include: 1 damage to the thyroid gland in the neck 2 erosion of the trachea, which is rare 3 lung collapse 4 scar tissue in the trachea
Why do people cover their tracheostomy tubes?
This is because the air you breathe no longer passes through your voice box. For some people, covering the tube helps them talk. Alternately, special valves can be attached to the tracheostomy tube. While still taking in air through the tube, these valves allow air to exit the mouth and nose, permitting speech.
Can a tracheostomy cause an allergic reaction?
Every medical procedure where the skin is broken carries the risk of infection and excessive bleeding. There’s also a chance of an allergic reaction to anesthesia, although it’s rare. Tell your doctor if you’ve had an allergic reaction to anesthesia in the past. Risks specific to a tracheostomy include: damage to the thyroid gland in the neck.
Can you put a tracheostomy tube in a ventilator?
The hole is then opened wide enough to fit a tracheostomy tube inside. Your doctor may hook up the tube to a ventilator, in case you need a machine to breathe for you. The tube will be secured in place with a band that goes around your neck. This helps keep the tube in place while the skin around it heals.