What is burn shock in burn injury?
Description of the problem Burn shock occurs in a major burn injury (covering >20% total body surface area [TBSA]) with disruption of normal organism homeostasis. This disruption is secondary to both local and systemic responses, including release of cytokines and other inflammatory mediators.
How does burn shock affect the cardiovascular system?
However, it is now realized that burn shock is a complex process not only affecting preload but also influencing cardiac output and systemic vascular resistance. During the first 8 hours after thermal injury a substantial increase in capillary permeability occurs resulting in a state of intravascular volume depletion.
What is considered a major burn?
Description of the problem Major burns can be devastating injuries. They have historically been defined as >20% total body surface area (TBSA), as this level of tissue destruction is associated with increased capillary leak and release of inflammatory cytokines, which can result in hypovolemia and shock without appropriate and timely intervention.
What is the prognosis of burn shock?
Early and adequate resuscitation of major burns has been the foundation to improving survival of burn patients with burn shock. The maintenance of ECF volume, until capillary integrity and cardiovascular function recover spontaneously 24-36 hours post-injury, is life-saving but has very little effect on the pathophysiologic course of burn shock.
See more
What type of shock can result from severe burns?
Burn shock is a term used to describe certain signs such as: decreased cardiac output, increased vascular resistance, hypovolaemia and hypoperfusion that occur after severe burn injuries have been sustained.
What are complications of a major burn?
Complications of deep or widespread burns can include: Bacterial infection, which may lead to a bloodstream infection (sepsis) Fluid loss, including low blood volume (hypovolemia) Dangerously low body temperature (hypothermia)
Is shock a complication of burns?
Burns and scalds can sometimes lead to further problems, including shock, heat exhaustion, infection and scarring.
What is the most immediate threat to life from a serious burn?
Dehydration. In severe or widespread burns, fluid is lost through the skin, and the person can become dehydrated. Dehydration can lead to life-threatening shock. A doctor will treat dehydration with intravenous (IV) fluids.
What are the two most life threatening concerns about severe burns?
Severe burns can result in many complications that affect the health of a victim and may even become fatal. The most life-threatening concerns for a burn injury are: Infection. Shock.
What are the 5 most important factors to consider in severity of burns?
How is the severity of burn assessed?Degree (depth) of the burn,Size (percentage) of the skin that is burned, and.Age of the injured person.Other factors include: Location of the burn on the body, Inhalation of toxic gases or smoke, Type of burn, Other traumatic injuries (bone fractures), and.
What type of complications may occur with a third degree burn?
Third Degree Burn Complications Hypothermia, or dangerously low body temperature, may also occur. During the healing process, infection is one of the most common complications of third degree burn. In cases of severe infection, the patient may develop sepsis. Sepsis can lead to shock and organ failure.
What are the major problems that occur with 3rd degree burns?
Potential complications of third-degree burns include:Arrhythmia, or heart rhythm disturbances, caused by an electrical burn.Dehydration.Disfiguring scars and contractures.Edema (excess fluid and swelling in tissues).Organ failure.Pneumonia.Seriously low blood pressure (hypotension) that may lead to shock.More items...•
What is burn shock?
Burn shock occurs in a major burn injury (covering >20% total body surface area [TBSA]) with disruption of normal organism homeostasis. This disruption is secondary to both local and systemic responses, including release of cytokines and other inflammatory mediators. Burn shock is similar to an ischemia-reperfusion injury that manifests at a cellular level and then systemically.
What happens when a burn size exceeds 20%?
When burn size exceeds 20% TBSA, heat injury releases cytokines, inflammatory mediators that increase capillary leak, and severe hypoproteinemia ensues. This causes intravascular volume shifts with resultant interstitial edema formation, vascular volume depletion and electrolyte imbalance. Isotope dilution studies have demonstrated up to 50% loss of ECF in unresuscitated burn shock. This intravascular depletion is associated with decreased cardiac output and increased pulmonary and systemic vascular resistance and results in shock.
What is the volume of isotonic crystalloid fluid necessary to maintain extracellular fluid and cardiovascular function during burn shock?
The volume of isotonic crystalloid fluid necessary to maintain extracellular fluid (ECF) volume and cardiovascular function during burn shock is in the range of 2-4 mL/kg per percent TBSA of second- and third-degree burns in the first 24 hours post-injury for 80-95% of patients. Increased volume resuscitation requirements are associated with inhalational injury, electrical burn, full-thickness injury with extensive tissue trauma and a delay in resuscitation (considered to be >2 hours post-injury).
How does colloidal resuscitation affect the oncotic pressure?
Large-volume crystalloid resuscitation in burn shock exacerbates the low oncotic pressure by decreasing the plasma protein concentration further, thus promoting local and systemic edema formation. Colloid resuscitation may replenish the intravascular oncotic pressure and limit the ensuing tissue edema. Capillary integrity, which is restored at 24 hours, may allow for the manipulation of intravascular oncotic pressure by administration of colloid. Studies have shown little clinical benefit of colloid resuscitation in first 12 hours post-injury with an increase in lung water in the post-resuscitation phase. Most U.S. burn centers will add albumin to the resuscitation 17-24 hours following the injury with a TBSA burn >40%.
How long after burn to give colloid infusion?
Rescue colloid infusions after 24 hours after burn or after 12 hours following injury if resuscitation requirements exceed 120% normal
How long does it take to resuscitate after a burn?
The first 48 hours following injury are focused on acute resuscitation with patient assessment, airway protection and fluid replacement. Optimal resuscitation aims to minimize rather than treat burn shock by maintenance of organ perfusion with the least amount of fluid necessary. Most patients with burn shock can be resuscitated successfully using various fluid regimens as demonstrated by multiple different resuscitation guidelines, mostly based on body weight and burn size. Radioisotope experiments by Baxter and Pruitt have shown that plasma expansion during early resuscitation was independent of the type of fluid given. The question of optimal fluid resuscitation (volume and type) remains open for debate. While under-resuscitation leads to decreased perfusion, acute kidney injury and ultimately death, over-resuscitation is also associated with complications, such as edema formation, abdominal compartment syndrome, acute respiratory distress syndrome, and multiple organ dysfunction.
How common are burns?
Burns are a major problem in the developed and developing world. They are common, devastating both physically and psychologically, and span the entire age spectrum. A 10-year review from the National Burn Repository published in 2006 showed 125,000 acute burn admissions to U.S. burn centers per annum. Of these admissions, 70% were male, with a mean age of 33 years; 10% were infants; and 8.5% were >70 years of age. Only 10% of patients had a burn size >30% TBSA, and inhalational injury was reported in 6.5% of patients. Flame and scald burns account for 78% of total cases, with 43% of these injuries occurring in the home and only 17% being work-related.
What causes burn shock?
Pathophysiology of Burn Shock. The interaction between hypovolaemia, direct tissue and anti-inflammatory substances in the body cause burn shock. Soon after burn injuries occur, Starling forces which determine the directionality of net water movement between different compartments begin to allow fluid to move from blood to both tissues ...
What is burn shock?
Burn shock is a term used to describe certain signs such as: decreased cardiac output, increased vascular resistance, hypovolaemia and hypoperfusion that occur after severe burn injuries have been sustained.
How long does it take for a burn to shock you?
Burn shock mostly occurs within the first 24hrs after sustaining burn injuries with its peak levels at 6 to 8 hours after the injury.
Why do burns cause oedema?
The formation of oedema (increased interstitial fluid) that soon follows burn injuries is mainly due to the creation of a strong negative interstitial fluid pressure and increased capillary permeability (otherwise known as capillary leakage syndrome).
Is burn shock better prevented or minimized than treated?
Burn shock is better prevented or minimized than treated . The administration of fluid resuscitation promptly, within the first 24hrs of the occurence of burn injuries is crucial, especially when burns are extensive and above 20% of the total burn surface area in both adults and children.
Can a physiotherapist handle burn shock?
Physiotherapists may not be directly involved in the management of burn shock but, it is pertinent to still have a knowledge about it since we will be involved in the rehabilitation of patients with burn injuries from their inception into the burn care unit.
Is burn shock better than fluid resuscitation?
Burn shock is better prevented or minimized than treated. The administration of fluid resuscitation promptly, within the first 24hrs of the occurence of burn injuries is crucial, especially when burns are extensive and above 20% of the total burn surface area in both adults and children. Fluid resuscitation is primarily aimed at the maintenance of vital organ function while also avoiding the complications that may stem from over and under resuscitation. The Parkland formula is mostly used to determine the amount of fluid to infuse. It is given as:
How does a burn affect the body?
Burn injuries induce a hypermetabolic response, which can increase the basal metabolic rate by more than 100%. Patients with major burns are at risk of developing protein calorie malnutrition with associated poor wound healing, immune suppression and infection; most require supplementation despite robust oral intake. Enteral feeding can be started as early as 12 hours post-burn, and has been linked to reduced wound infection risk, enhanced wound healing and shorter hospital length of stay in both adult and pediatric populations. Other therapies proposed for reducing the catabolism of burn injuries include anabolic steroids such as oxandrolone, and the beta blocker propranolol.
What is the diagnosis of a major burn?
Diagnosis of a major burn must be done in correlation with a thorough history of the events leading up to the injury, including knowledge of the mechanism, its qualitative specifics (e.g. type of liquid in a scald injury, or level of voltage in an electrical injury), as well as the timing of the burn.
What is TBSA in burn trauma?
Burn Trauma. 1. Description of the problem. Major burns can be devastating injuries. They have historically been defined as >20% total body surface area (TBSA), as this level of tissue destruction is associated with increased capillary leak and release of inflammatory cytokines, which can result in hypovolemia and shock without appropriate ...
How common are burns?
They are common, they are devastating both physically and psychologically, and they span the entire age spectrum. A 10-year review from the National Burn Repository published in 2010 showed 148,419 acute burn admissions to U.S. burn centers. Of these admissions, 70% were male, with a mean age of 32 years, 17% were <5 years of age and 12% were >60 years of age. Only 36.7% of patients had a major burn (> 20%TBSA), and inhalational injury was reported in 5.9% of patients. Flame and scald burns accounted for 72% of total cases. 66% of burn injuries occur in the home, with only 14.6% being work-related. The average length of hospital stay declined over the past 10 years from 11 to 9 days, and can be predicted as 1 day for every %TBSA burned.
How to treat a burn wound?
Treatment of burns begins with hydrotherapy. The wounds are washed with warm water and chlorhexidine and debrided of any necrotic or loose tissue, and blisters are deroofed. Topical antimicrobials and occlusive dressings, such as cling or mesh gauze, and a compressive elastic wrap in the case of extremity burns, are applied. This is done to prevent any further progression of tissue damage or desiccation. Common topical antimicrobials are as follows:
Which type of injury poses the greatest risk of morbidity or mortality?
Any patient with burns and concomitant trauma (such as fracture) in which the burn injury poses the greatest risk of morbidity or mortality
Is it necessary to estimate the depth of a burn?
Estimation of Burn Depth. Estimation of burn depth is not required for immediate resuscitation needs, but is very important when planning future surgical intervention. Burns are dynamic wounds, and depth can vary depending on time of exposure, contact temperature, skin thickness, and adequacy of resuscitation.
What are the complications of a deep burn?
Complications of deep or widespread burns can include: Bacterial infection, which may lead to a bloodstream infection (sepsis) Fluid loss, including low blood volume (hypovolemia) Dangerously low body temperature (hypothermia) Breathing problems from the intake of hot air or smoke.
What is a second degree burn?
Second-degree burn. A second-degree burn, which often looks wet or moist, affects the first and second layers of skin (epidermis and dermis). Blisters may develop and pain can be severe. Burns are tissue damage that results from heat, overexposure to the sun or other radiation, or chemical or electrical contact.
What causes burns in the airway?
Burns caused by chemicals or electricity. Difficulty breathing or burns to the airway. Take first-aid measures while waiting for emergency assistance. Call your doctor if you experience: Signs of infection, such as oozing from the wound, increased pain, redness and swelling.
What does a 3rd degree burn look like?
Deep second-degree burns can cause scarring. 3rd-degree burn. This burn reaches to the fat layer beneath the skin. Burned areas may be black, brown or white. The skin may look leathery.
What is the difference between 1st degree burn and 2nd degree burn?
1st-degree burn. This minor burn affects only the outer layer of the skin (epidermis). It may cause redness and pain. 2nd-degree burn. This type of burn affects both the epidermis and the second layer of skin (dermis). It may cause swelling and red, white or splotchy skin. Blisters may develop, and pain can be severe.
What causes ridged scars?
Breathing problems from the intake of hot air or smoke. Scars or ridged areas caused by an overgrowth of scar tissue (keloids) Bone and joint problems , such as when scar tissue causes the shortening and tightening of skin, muscles or tendons (contractures)
Can you rub a potato on a burn?
Is it ok/recommended to rub the inside of an uncooked potato on a burn? Unfortunately this is definitely a first aid myth! The priority with a burn is to cool the area to prevent further damage to the tissues. This is best achieved by using cool running water for at least 10 minutes.
Can you cool a burn?
The priority is definitely cooling the burn as this will reduce the tissue damage and slow the burning process. Infection is a longer term complication which can be managed by health care professionals later in the healing process. So yes – improvise with any water available!

Description of The Problem

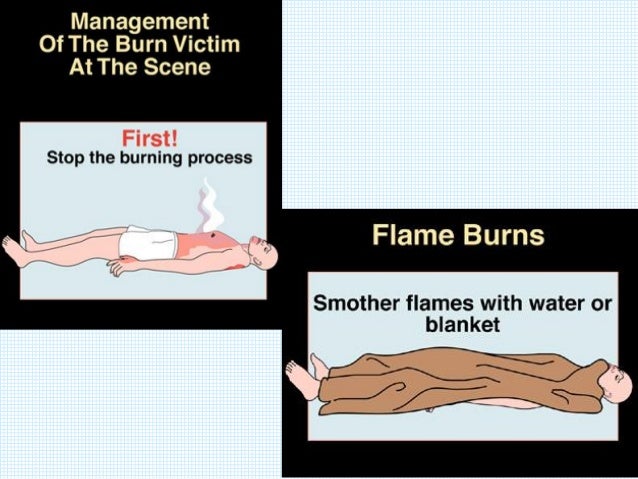
Emergency Management
- Fluid resuscitation is focused on supporting the patient through the first 24-48 hours of profound hypovolemia and cardiac dysfunction following the thermal injury. The National Institutes of Health consensus stated that the minimum fluid resuscitation required to maintain adequate organ perfusion should be provided. This volume infused should be titrated to avoid either over- or und…
Diagnosis
- The Lund-Browder Chart (Figure 1) is usually completed at the time of admission to calculate the TBSA of the burn. If TBSA burned is >20%, or associated with an inhalational injury, electrical injury, trauma or a full-thickness burn it will likely result in burn shock if the patient is not promptly and adequately resuscitated. Most clinicians overestimate the size and depth of a burn, which m…
Specific Treatment
- Effective fluid resuscitation is one of the cornerstones of modern burn care and strives to mitigate the effect of burn shock. Patients with burns >20% TBSA should undergo guided fluid resuscitation based on body size and surface area burned. Most burn centers follow a variant of the Parkland resuscitation formula, now also known as the Consensus formula. Most guided res…
Disease Monitoring, Follow-Up and Disposition
- Effective resuscitation of burn shock will not achieve complete normalization of physiologic variables, as the burn injury leads to ongoing cellular and hormonal responses. Consequences of excessive resuscitation – pulmonary edema, myocardial edema, conversion of superficial to deep burns, need for fasciotomies in unburned limbs and abdominal compartment syndrome – are det…
Pathophysiology
- Burn shock at the cellular level occurs immediately following the thermal or chemical injury and is manifest by a decreased cellular membrane ATP-ase activity and reduced transmembrane potential. This results in increased intracellular sodium and extracellular potassium concentrations, leading to cellular swelling and acidosis in both injured and non-injured tissue. L…
Epidemiology
- Burns are a major problem in the developed and developing world. They are common, devastating both physically and psychologically, and span the entire age spectrum. A 10-year review from the National Burn Repository published in 2006 showed 125,000 acute burn admissions to U.S. burn centers per annum. Of these admissions, 70% were male, with a mean …
Prognosis
- Survival has remained at 95%, with deaths from burn injury increased at the extremes of age, increasing burn size, and the presence of inhalational injury. The leading cause of death was multiple organ failure complicated by pneumonia, wound infection and cellulitis. Risk factors for mortality include age >60 years, TBSA burn >40%, and inhalational injury, with a predicted mort…
What's The Evidence?
- Hettiaratchy, S, Papini, R. “ABC of burns”. BMJ. vol. 328. 2004. pp. 1555-7. Pham, TN, Cancio, LC, Gibran, NS. “American Burn Association Practice Guidelines: Burn Shock Resuscitation”. J Burn Care Res. vol. 29. 2008. pp. 257-65. Lee, MA. “Role of gut-lymph factors in the induction of burn-induced and trauma-shock induced acute heart failure”. Int J Clin Exp Med. vol. 1. 2008. pp…