Common Causes
Most of the time, oliguria can be treated at home, but in some cases, it can be a symptom of a serious medical condition that requires further testing and treatment. Oliguria is different from anuria, which is when urine output stops completely. The primary symptom of oliguria is producing less urine than normal.
Related Conditions
The management of postoperative oliguria should aim to restore urine output and to treat the underlying disorder. Once urine output is adequate, the underlying cause of the oliguria must be considered. This is commonly a result of hypovolaemia.
Can oliguria be treated at home?
The primary symptom of oliguria is producing less urine than normal. Individuals might experience other symptoms as well, depending on the cause of the decrease. Urine that is a darker color than normal (generally a deeper yellow color such as amber) If there is red or dark red blood in urine, this is a different issue called hematuria .
What are the treatment options for postoperative oliguria?
Patients with renal failure that cannot be reversed may require renal replacement therapy (eg, continuous venovenous hemofiltration or hemodialysis). Categories of causes of oliguria include decreased renal blood flow, renal insufficiency, and urinary outflow obstruction.
What are the symptoms of oliguria?
What are the treatment options for oliguria in renal failure?
How does oliguria affect the prognosis?
What is oliguria in renal function?
What to do if fluid resuscitation fails?
What causes oliguria in the kidney?
Is oliguria a physiological condition?
Is oliguria a prerenal or postrenal condition?
Does oliguria cause fluid overload?
See 4 more
About this website
How do you treat oliguria?
A simple way to treat oliguria is by increasing the amount of fluids you take in. This can often be done at home by drinking more water or rehydration solutions that include electrolytes.
What medication is used to treat oliguria?
Drugs used to treat OliguriaDrug nameRatingRx/OTCGeneric name: furosemide systemic Drug class: loop diuretics For consumers: dosage, interactions, side effects For professionals: Prescribing InformationExpand current row for information about mannitol mannitolRateRx10 more rows
How do you assess for oliguria?
Imaging studies in oliguria include the following: Renal ultrasonography. Voiding cystourethrography - Indicated for suspected bladder outlet obstruction. Radionuclide renal scanning - May be useful in the assessment of transplant rejection and obstruction.
What amount of urine is oliguria?
Oliguria is defined as a urine output that is less than 1 mL/kg/h in infants, less than 0.5 mL/kg/h in children, and less than 400 mL daily in adults.
What organ is affected by oliguria?
[1] Oliguria can arise as a result of the normal physiological response of the body or due to an underlying pathology affecting the kidney or urinary tract. The human body has a normal physiological mechanism of conserving fluids and electrolytes in episodes of hypovolemia.
How can I increase my urine output?
Nine ways to induce urinationTapping the area between navel and pubic bone. ... Bending forward. ... Placing a hand in warm water. ... Running water. ... Drinking while trying to urinate. ... Trying the Valsalva maneuver. ... Exercising. ... Massaging the inner thigh.More items...•
What do nurses do with low urine output?
Oliguria (poor urine output) is a common sign of critical illness and is associated with poor fluid intake or excessive fluid loss....Registered nurses responsible for patients should be able to:Interpret fluid balance;Administer intravenous fluids as prescribed;Insert a urinary catheter (Department of Health, 2008).
What causes very little urine output?
Common causes include: Dehydration from not drinking enough fluids and having vomiting, diarrhea, or fever. Total urinary tract blockage, such as from an enlarged prostate. Medicines such as anticholinergics and some antibiotics.
Can dehydration cause low urine output?
Dehydration. Share on Pinterest Dehydration is a common cause of low urine output. One of the more common causes of low urine output is dehydration. Dehydration occurs when the body does not get enough liquid from the diet or is releasing liquid too fast for a person to replenish it.
What medications cause low urine output?
Medicines: Certain drugs can make you pee less, including:Nonsteroidal anti-inflammatories (NSAIDs), like aspirin and ibuprofen.Certain antibiotics.Some chemotherapy drugs.ACE inhibitors to control blood pressure.Medications used to treat overactive bladder.More items...•
How long can you go without passing urine?
When you hold your pee for 10 hours or more, you may develop urinary retention, meaning the muscles in your bladder can't relax and let you relieve yourself, even when you want to. In very rare cases, holding your pee can cause your bladder to burst.
What medications cause difficulty urinating?
Urinary retention can also be caused by certain medications. Drugs like antihistamines (Benadryl®), antispasmodics (like Detrol®), opiates (like Vicodin®) and tricyclic antidepressants (like Elavil®) can change the way the bladder muscle works.
How is anuria treated?
The exact treatment for anuria depends on the underlying condition that's causing it. Kidney disease may be treated with dialysis to remove fluids and waste. Ureteral stents may also help collect urine. A kidney transplant is considered a last resort.
Which descriptor of urination is associated with the term oliguria quizlet?
Dysuria. Nocturia. Oliguria. Normal urine output is about 2500 mL per day. The patient's urine output is less than 400 mL per day, which indicates oliguria (a condition in which the patient has reduced urine output).
Oliguria (Low Urine Output): Causes, Symptoms & Treatment
Symptoms and Causes What causes oliguria? Oliguria (low urine output) can be pre-renal (caused by something happening before the waste process gets to your kidneys), renal (caused by something in your kidneys) or post-renal (caused by something happening later in the waste removal process, not in your kidneys.)
Oliguria Causes & Symptoms | What is Oliguria? | Study.com
Oliguria. Joe has noticed in the last day that he has gone to the bathroom only once, and is barely passing any urine. He is not aware of it yet, but what he is experiencing is called oliguria.
What Is Oliguria and Anuria? - MedicineNet
Renal or kidney failure is a condition in which the kidney is unable to perform its function properly. This condition may be temporary or permanent. There are two different types of kidney failure: Acute kidney injury: It may start suddenly and may be reversible.It may occur due to injury, infections, medication side effects, or pre-existing diseases.
Oliguria: Causes, Diagnosis, and Treatment - WebMD
SOURCES: Korean Journal of Critical Care Medicine: “The Role of Oliguria and the Absence of Fluid Administration and Balance Information in Illness Severity Scores.” Medscape: “Oliguria ...
How does oliguria affect the prognosis?
The duration and intensity of oliguria have a great impact on prognosis. As the intensity of oliguria worsens to <0.5 ml/kg/h, the mortality rises significantly. [4]
What is oliguria in renal function?
Oliguria is defined as urinary output less than 400 ml per day or less than 20 ml per hour and is one of the earliest signs of impaired renal function .[1] It had been described early in the literature when Hippocrates identified the prognostic importance of the urinary output. It was in the second century that Galen proposed its significance to indicate renal function.[2] Later on, renal failure accompanied by oliguria was described by Heberden as ‘ischuria renalis.’[3][4] According to the Acute Dialysis Quality Initiative group, a patient with urinary output <0.3 ml/kg/h for at least 24 hours can be defined to be oliguric.[5]
What to do if fluid resuscitation fails?
If fluid resuscitation fails to resolve the oliguria , diure tic therapy should be initiated utilizing a standardized approach. A furosemide stress test (FST) can be done in order to assess the patient’s response to diuresis. It should be noted that a diuretic challenge should only be given once the patient is euvolemic. Failure of resolution of oliguria with the above step(s) should raise suspicion for evaluation for acute kidney injury (AKI). FST is a standardized test to assess the functional integrity of the tubules and aids in the risk stratification as well as decision making. FST is said to be nonresponsive if 1.0-1.5 mg/kg of furosemide produces a urine output of 100 ml/h in the first two hours. Nonresponsive FST is associated with a higher stage of AKI. Some studies suggest using 100-200 mg of furosemide initially, and if there is no response, doubling the dose may be considered. If this fails to bring any significant improvement adding a thiazide diuretic can also be considered. [1]
What causes oliguria in the kidney?
Renal causes of oliguria arise as a result of tubular damage. As a result of the tubular damage, the kidney loses its normal function i.e., production of urine while excreting the waste metabolites. In addition to this, direct damage to the renal tubules leads to a back leak of filtered uremic metabolites from the tubular lumen into the bloodstream. Hence, in these cases, decreased production of urine leads to oliguria.
Is oliguria a physiological condition?
Oliguria can be the result of various causes that can be apparent or subclinical.[1] Oliguria can arise as a result of the normal physiological response of the body or due to an underlying pathology affecting the kidney or urinary tract. The human body has a normal physiological mechanism of conserving fluids and electrolytes in episodes of hypovolemia. These mechanisms are under close neurohormonal control and are completely reversible without any subsequent injury to the kidneys.[6] The various etiologic factors can be broadly classified into prerenal, renal, and postrenal causes depending upon the pathophysiology.
Is oliguria a prerenal or postrenal condition?
Oliguria is a frequently encountered clinical condition that can arise due to either prerenal, renal, or post-renal abnormalities. It has various etiologies and management is dependent on the underlying cause(s). In order to avoid renal failure, the providers should not only keep in view the etiology and management of oliguria but also the various risk factors and precipitating factors as well. This activity reviews the evaluation and management of oliguria and highlights the role of the interprofessional team in improving care for patients with this condition.
Does oliguria cause fluid overload?
It should be kept in mind that in the setting of oliguria, fluid resuscitation does put the patient at risk of fluid overload, which in turn leads to worse ning AKI. As a result, overcompensation with fluid is associated with higher mortality when urine output is the determining factor for fluid replacement.[15] Signs of fluid overload include peripheral edema, increased CVP, and increased IVC diameter. [16][17] In diuretic responsive patients with fluid overload, diuretic medications are used to manage the fluid overload. On the other hand, in patients who are nonresponsive to diuretics, renal replacement therapy can be used. [3][12]
How to prevent oliguria?
Because many cases of oliguria are caused by dehydration, one of the best ways to prevent it is by taking in enough fluids. The amount of fluids you need to drink will depend on how much you’re losing through sweat or sickness, as well as your overall diet.
What is the best medicine for oliguria?
Medications used to treat oliguria include: Antimicrobials: To treat infections, such as those that cause serious diarrhea or vomiting. Diuretics: Which force the body to produce more urine. In small amounts, diuretics can help increase urine output, but as noted above, too much can backfire and make oliguria worse.
How much urine do you need to have oliguria?
Doctors diagnose oliguria based on the amount of urine you produce in a day, though the criteria used are different for adults and kids: Adults: less than 500 milliliters (mL) of urine in a 24-hour period. 2 . Children: less than 500 mL/1.73 square meter (m2) in a 24-hour period.
What is the difference between anuria and oliguria?
Oliguria is different from anuria, which is when urine output stops completely.
How is oliguria diagnosed?
Oliguria is typically diagnosed during a physical exam. Healthcare providers also might want to run further tests to investigate potential causes or check for related health issues.
How do you know if you have oliguria?
The primary signs and symptoms of oliguria are: 1 . Urinating less frequently and/or producing a smaller amount than usual . Urine is a darker color than normal (generally a deeper yellow color such as amber).
How to treat fluid retention?
Generally speaking, healthcare providers typically recommend increasing your fluid intake, stopping medications that may be causing the problem, and/or using medications to treat the problem. 2
What is the etiology of oliguria?
Etiology of Oliguria. Causes of oliguria are typically divided into 3 categories: There are numerous such entities (see Acute Kidney Injury ), but a limited number cause most cases of acute oli guria in hospital ized patients (see table Some Causes of Oliguria ).
What electrolytes are used to determine the cause of oliguria?
Serum electrolytes such as sodium, blood urea nitrogen and creatinine should be measured to assist in determining the cause of oliguria. A high ratio of serum BUN to creatinine (eg, > 20:1) suggests a prerenal cause.
What is the best treatment for oliguria?
In serious cases, you may need a transplant or dialysis, a process that takes out extra water and toxins from your blood since your kidneys can’t.
How to treat oliguria?
The treatment for oliguria depends on the cause. If you're dehydrated, your doctor will recommend that you drink more fluids and electrolytes. In serious cases, you may need fluids through an IV (a tube that puts fluid directly into a vein in your hand or arm).
What causes a person to pee less?
Medicines: Certain drugs can make you pee less, including: Kidney disease : Oliguria can cause kidney failure, but more often it’s a symptom that your kidneys aren’t working the way they should.
Why does oliguria go away?
Causes. Lots of different things can cause oliguria. Many of them go away on their own, but some need medical treatment. Dehydration: This is the most common cause of oliguria. It happens most often when you've been vomiting or had diarrhea. Burns and other serious injuries: Burns can dehydrate you and make you pee less.
Can oliguria cause kidney failure?
Kidney disease: Oliguria can cause kidney failure, but more often it’s a symptom that your kidneys aren’t working the way they should.
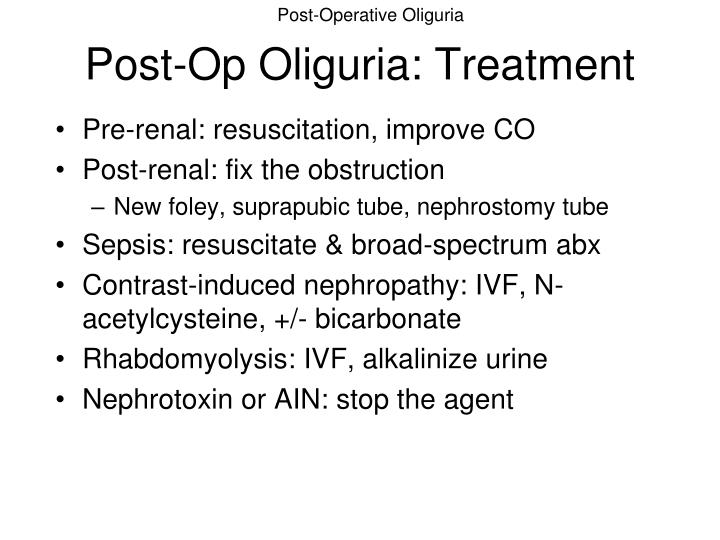
What should postoperative oliguria aim to do?
The management of postoperative oliguria should aim to restore urine output and to treat the underlying disorder. Once urine output is adequate, the underlying cause of the oliguria must be considered.
What causes oliguria in the postoperative period?
Causes of oliguria in the postoperative period are conveniently subdivided into prerenal, renal, and postrenal causes. w2 Prerenal hypovolaemia is the most common cause of postoperative oliguria. It usually stems from inadequate management of fluids perioperatively because perioperative fluid losses are often underestimated.
What is the urine output of oliguria?
In practice this equates to a urine output of less than 0.5 ml/kg/hr for at least two consecutive hours or a daily urine output of less than 400 ml/day (about 15 ml/hr). w1w2
How to restore urine output in hypovolaemia?
This is commonly a result of hypovolaemia. To restore urine output in hypovolaemia fluid boluses are given. This mustbe followed by reassessment of the patient. Colloid solutions are commonly used, as they remain longer in the intravascular space because of their high oncotic pressure. A typical bolus volume in adults is 250 ml given over 30 minutes, although smaller volumes should be given to elderly people and to patients with a history of heart disease. w1w2 Bear in mind that it is poor practice to prescribe fluids together with a diuretic; diuretics are used to treat fluid overload but not hypovolaemia.
How to know if urine is inadequate?
Look at the fluid chart to confirm that the urine output is inadequate—that is, less than 0.5 ml/kg/hr for two consecutive hours. w1 Note the overall fluid balance. If there is no urine output at all (anuria), the urinary catheter may be blocked. Ask a nurse to flush the urinary catheter to ensure its patency. w2
Can angiotensin converting enzyme inhibitors cause prerenal oliguria?
Drugs that interfere with regulation of renal perfusion, such as angiotensin converting enzyme inhibitors, may also cause prerenal oliguria. Intrinsic renal disease may be induced by nephrotoxic drugs or result from a prolonged period of hypovolaemia.
Can hypovolaemia be compensated for by fluid shift?
Although hypovolaemia can to some degree be compensated for by fluid shift from the interstitium into the circulation, large fluid losses will ultimately drain the circulation.
How does oliguria affect the prognosis?
The duration and intensity of oliguria have a great impact on prognosis. As the intensity of oliguria worsens to <0.5 ml/kg/h, the mortality rises significantly. [4]
What is oliguria in renal function?
Oliguria is defined as urinary output less than 400 ml per day or less than 20 ml per hour and is one of the earliest signs of impaired renal function .[1] It had been described early in the literature when Hippocrates identified the prognostic importance of the urinary output. It was in the second century that Galen proposed its significance to indicate renal function.[2] Later on, renal failure accompanied by oliguria was described by Heberden as ‘ischuria renalis.’[3][4] According to the Acute Dialysis Quality Initiative group, a patient with urinary output <0.3 ml/kg/h for at least 24 hours can be defined to be oliguric.[5]
What to do if fluid resuscitation fails?
If fluid resuscitation fails to resolve the oliguria , diure tic therapy should be initiated utilizing a standardized approach. A furosemide stress test (FST) can be done in order to assess the patient’s response to diuresis. It should be noted that a diuretic challenge should only be given once the patient is euvolemic. Failure of resolution of oliguria with the above step(s) should raise suspicion for evaluation for acute kidney injury (AKI). FST is a standardized test to assess the functional integrity of the tubules and aids in the risk stratification as well as decision making. FST is said to be nonresponsive if 1.0-1.5 mg/kg of furosemide produces a urine output of 100 ml/h in the first two hours. Nonresponsive FST is associated with a higher stage of AKI. Some studies suggest using 100-200 mg of furosemide initially, and if there is no response, doubling the dose may be considered. If this fails to bring any significant improvement adding a thiazide diuretic can also be considered. [1]
What causes oliguria in the kidney?
Renal causes of oliguria arise as a result of tubular damage. As a result of the tubular damage, the kidney loses its normal function i.e., production of urine while excreting the waste metabolites. In addition to this, direct damage to the renal tubules leads to a back leak of filtered uremic metabolites from the tubular lumen into the bloodstream. Hence, in these cases, decreased production of urine leads to oliguria.
Is oliguria a physiological condition?
Oliguria can be the result of various causes that can be apparent or subclinical.[1] Oliguria can arise as a result of the normal physiological response of the body or due to an underlying pathology affecting the kidney or urinary tract. The human body has a normal physiological mechanism of conserving fluids and electrolytes in episodes of hypovolemia. These mechanisms are under close neurohormonal control and are completely reversible without any subsequent injury to the kidneys.[6] The various etiologic factors can be broadly classified into prerenal, renal, and postrenal causes depending upon the pathophysiology.
Is oliguria a prerenal or postrenal condition?
Oliguria is a frequently encountered clinical condition that can arise due to either prerenal, renal, or post-renal abnormalities. It has various etiologies and management is dependent on the underlying cause(s). In order to avoid renal failure, the providers should not only keep in view the etiology and management of oliguria but also the various risk factors and precipitating factors as well. This activity reviews the evaluation and management of oliguria and highlights the role of the interprofessional team in improving care for patients with this condition.
Does oliguria cause fluid overload?
It should be kept in mind that in the setting of oliguria, fluid resuscitation does put the patient at risk of fluid overload, which in turn leads to worse ning AKI. As a result, overcompensation with fluid is associated with higher mortality when urine output is the determining factor for fluid replacement.[15] Signs of fluid overload include peripheral edema, increased CVP, and increased IVC diameter. [16][17] In diuretic responsive patients with fluid overload, diuretic medications are used to manage the fluid overload. On the other hand, in patients who are nonresponsive to diuretics, renal replacement therapy can be used. [3][12]