Horizontal canal benign paroxysmal positional vertigo in a fighter pilot
- Abstract. Benign paroxysmal positional vertigo (BPPV) is the most common disorder of the peripheral vestibular system, characterized by intense, positional provoked vertigo.
- Introduction. Vertigo is the illusion of motion, usually rotational motion. ...
- Case Report. ...
- Discussion. ...
- Conclusion. ...
- Footnotes. ...
- References. ...
What is HC-BPPV (horizontal canal benign paroxysmal positional vertigo)?
Horizontal canal benign paroxysmal positional vertigo, or HC-BPPV, is a common condition in the elderly. It normally occurs when fluid builds up inside the horizontal semicircular canal in your inner ear, but it may also be caused by neurological or cardiac problems. [1]
What is the most common variant of benign paroxysmal positional vertigo (BPPV)?
Lateral (horizontal) canal BPPV is the most common atypical variant, accounting for about 3 percent of cases. Most cases are seen as a consequence of canalith repositioning therapy Lateral Canal BPPV is diagnosed by demonstration of a horizontal nystagmus that changes direction depending on the ''down'' ear.
What is HC-BPPV?
Horizontal canal benign paroxysmal positional vertigo, or HC-BPPV, is a common condition in the elderly. It normally occurs when fluid builds up inside the horizontal semicircular canal in your inner ear, but it may also be caused by neurological or cardiac problems.
What is the pathophysiology of BPPV?
BPPV occurs when free-floating otoconia move in one of the semicircular canals (canalithiasis) or by otoliths adhered to the cupula, which is the membrane located at one end of each semicircular canal (cupulolithiasis).

How do I fix horizontal BPPV?
3:325:15Log Roll Maneuver (Horizontal Canal BPPV Treatment) - YouTubeYouTubeStart of suggested clipEnd of suggested clipAll you can do is start by rolling side to side of bed start off on your. Back. You're going toMoreAll you can do is start by rolling side to side of bed start off on your. Back. You're going to quickly roll to your right engage how dizzy you get.
How common is horizontal canal BPPV?
BPPV originating from stimulation of the lateral semicircular canal is the second most common type of BPPV, accounting for approximately 5–15% of the patients but its frequency has been occasionally reported up to 30% [20, 32] Lateral canal BPPV is due to detached otoconia that enter the lateral canal instead of the ...
How do you test for BPPV horizontal canal?
2:205:03Supine Head Roll Test | Lateral BPPV - YouTubeYouTubeStart of suggested clipEnd of suggested clipThe clinician should perform a supine head roll test to assess for lateral. Also called horizontalMoreThe clinician should perform a supine head roll test to assess for lateral. Also called horizontal semicircular canal BPPV.
What causes horizontal vertigo?
It is usually triggered by specific changes in your head's position. This might occur when you tip your head up or down, when you lie down, or when you turn over or sit up in bed.
How long does it take for ear crystals to dissolve?
The results demonstrated that normal endolymph can dissolve otoconia very rapidly (in about 20 hours).
Which ear affects BPPV?
Benign paroxysmal positional vertigo (BPPV) is a problem in the inner ear. It is the most common cause of vertigo, which is a false sensation of spinning or movement.
Is BPPV caused by stress?
There is some evidence that prolonged stress and anxiety can actually lead to a specific vestibular disorder: BPPV (which is the most common cause of vertigo).
What is the fastest way to cure BPPV?
What is the fastest way to cure BPPV? The most effective benign paroxysmal positional vertigo treatments involve physical therapy exercises. The goal of these exercises is to move the calcium carbonate particles out of your semicircular canals and back into your utricle.
What is the best medication for BPPV?
In an emergency situation when a patient presents with intractable vertigo and vomiting, intravenous diazepam (Valium) may be useful in decreasing inflammation in the labyrinths. In less severe cases, over the counter medications like meclizine (Antivert, Bonine, Dramamine II, D-Vert) may be helpful.
Does BPPV cause horizontal nystagmus?
Horizontal/Lateral semicircular canal BPPV The 2 types of lateral semicircular canal BPPV have different nystagmus findings: Geotropic – elicits horizontal nystagmus that beats toward the earth when the patient head is rolled to the pathologic side.
Can drinking alcohol cause BPPV?
Alcohol can exacerbate the symptoms of preexisting hearing-related problems like Meniere's disease and BPPV, as well.
How is horizontal cupulolithiasis treated?
Conclusion: The cupulolith repositioning maneuver is an effective method for treating horizontal canal cupulolithiasis. It may also provide an insight into the side of the cupula where otoliths are attached.
What is the process of BPPV?
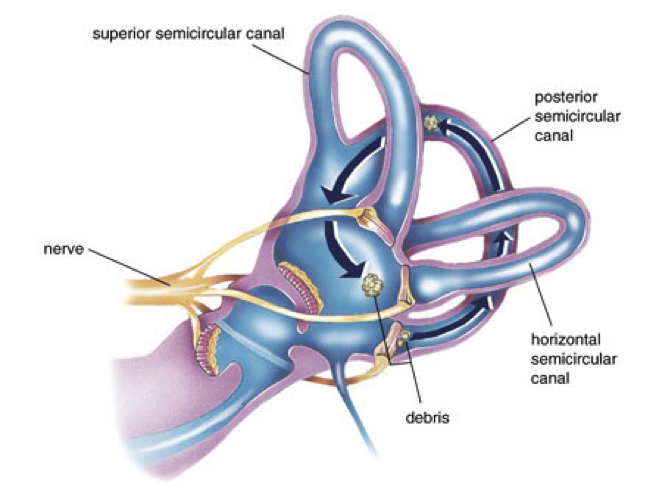
BPPV develops when calcium carbonate crystals, which are known as otoconia, shift into and become trapped within the semicircular canals ( one of the vestibular organs of the inner ear that control balance). The otoconia make up a normal part of the structure of the utricle, a vestibular organ next to the semicircular canals. (See illustration.)
What is the name of the condition where the head is spinning?
Benign paroxysmal positional vertigo (BPPV) is an inner ear disorder in which changes in the position of the head, such as tipping the head backward, lead to sudden vertigo – a feeling that the room is spinning. The vertigo sensation can range from mild to severe and usually lasts only a few minutes. It may be accompanied by other symptoms, ...
What is the name of the condition where the head is tipped backwards?
Benign paroxysmal positional vertigo (BPPV) is an inner ear disorder in which changes to the position of the head, such as tipping the head backward, lead to sudden vertigo – a feeling that the room is spinning. BPPV is not a sign of a serious problem. If it does not disappear on its own within 6 weeks, it can be treated with a short, ...
Why is the otoconia loosened?
(See illustration.) In the utricle, the otoconia may be loosened because of injury, infection, or age. They land in a sac – the utricle – where they are naturally dissolved.
How is BPPV diagnosed?
The diagnosis can usually be made in the office based on medical history and a physical exam. Treatment also involves a short, simple in-office procedure known as the particle repositioning maneuver. (See the treatment section).
How long does it take to do a particle reposition?
What is the particle repositioning procedure for benign paroxysmal positional vertigo (BPPV)? The particle repositioning procedure takes about 15 minutes to complete and involves a series of physical movements that change the position of the head and body.
What is the movement of the cilia that causes vertigo?
Vertigo develops when the cilia are stimulated by the rolling otoconia. Movements that can bring about an episode of BPPV include: Rolling over or sitting up in bed; Bending the head forward to look down, or; Tipping the head backward.
What brings on BPPV?
In many people, especially older adults, there is no specific event that causes BPPV to occur, but there are some things that may bring on an attack:
What is the Epley maneuver?
The Epley maneuver and other bedside physical therapy maneuvers and exercise programs can help reposition the crystals from the semicircular canals. Recurrences can occur, and repeat repositioning treatments are often necessary. After Epley maneuver treatment, the patient may begin walking with caution.
How to diagnose BPPV?
Diagnosing BPPV involves taking a detailed history of a person’s health. The doctor confirms the diagnosis by observing nystagmus — jerking of the person’s eyes that accompanies the vertigo caused by changing head position. This is accomplished through a diagnostic test called the Dix-Hallpike maneuver.
What nerve causes vertigo and jumping eyes?
The otoconia move to the lowest part of the canal, which causes the fluid to flow within the SCC, stimulating the balance (eighth cranial) nerve and causing vertigo and jumping eyes (nystagmus).
What does it feel like to spin with BPPV?
People with BPPV can experience a spinning sensation — vertigo — any time there is a change in the position of the head.
How long does it take for BPPV to go away?
Even without treatment, the usual course of the illness is lessening of symptoms over a period of days to weeks, and sometimes there is spontaneous resolution of the condition.
How long does BPPV last?
BPPV can affect people of all ages but is most common in people over the age of 60. Most patients can be effectively treated with physical therapy. In rare cases, the symptoms can last for years.
What to do if patient reacts violently during roll test?
If the patient reacts violently during the roll test, immediately turn the patient to the opposite side and perform a Lempert 360-degree roll.
How to tell if you have otoconia?
These symptoms might include, blurred vision, numbness, weakness of the arms or legs or confusion. 3. Allow enough time for otoconia displacement. It is important to remember that the consistency of fluid inside the vestibular system is viscous.
What position should a patient be in to guide the patient back into a neutral position?
Guide the patient back into a neutral, supine position.
When to use VNG goggles?
Video Frenzel or VNG goggles. It is most helpful to use Video Frenzel or VNG goggles when performing the roll test. This reduces the ability of the patient to fixate during the procedure to reduce the nystagmus response. This will also allow the examiner to see even very slight horizontal nystagmus. 5.
How much elevation of head is needed for a scuba diver?
A slight elevation of the head (approximately 20 degrees) is helpful.
What to know before a roll test?
1. Past injuries. Before performing the roll test, it is important to find out whether the patient has current or past injuries of the neck or spine. 2.
Which side of the body is worse, nystagmus or nystagmus?
Nystagmus is worse on the affected side and beats toward the ground.
Why does BPPV occur?
Though not fully understood, BPPV is thought to arise due to the displacement of otoconia (small crystals of calcium carbonate) from the maculae[1]of the inner ear into the fluid-filled semicircular canals. These semicircular canals are sensitive to gravity and changes in head position can be a trigger for BPPV[2].
How to test for canalithiasis of the posterior canal?
The most commonly used test is Dix-Hallpike which assesses involvement of the posterior canal (the most commonly affected semicircular canal). The test involves turning the head 45 degrees to the side being tested and then quickly moving from a seated to a supine position with the head declined 30 degrees below the trunk. The test must be performed quickly to ensure sufficient displacement of the endolymp and otoconia to provoke the expected symptoms. The test is considered positive for canalithiasis of the posterior canal if vertigo is provoked and nystagmus is observed, both of which should be of short-duration for canalithiasis. The direction of the observed nystagmus should be consistent with the canal being assessed. For the posterior canal, nystagmus should be up-beating and torsional in an ipsilateral direction (if testing the affected side. If the left side is affected but the test is performed with the head turned to the right, the nystagmus would be up-beating and torsional to the right).
What is the otoconia in the ear?
Within the labyrinth of the inner ear lie collections of calcium crystals known as otoconia. In patients with BPPV, the otoconia are dislodged from their usual position within the utricle and they migrate over time into one of the semicircular canals (the posterior canal is most commonly affected due to its anatomical position). When the head is reoriented relative to gravity, the gravity-dependent movement of the heavier otoconial debris (colloquially ear rocks or crystals) within the affected semicircular canal causes abnormal (pathological) fluid endolymph displacement in the affected ear. This fluid displacement will send a signal to the brain indicating that rotational movement is occuring. However, the vestibular apparatus in the unaffected ear will not be transmitting the same signal because there are no loose otoconia triggering the hair cells abnormally. This resultant mismatch in signals coming from the right and left vestibular systems lead to the sensation of vertigo. This more common condition is known as canalithiasis. Vertigo associated with this condition will be of short duration, even if the person with the condition stays in the provocative position, because the endolymph and otoconia will quickly come to a rest so the hair cells will no longer be displaced and triggering the signal to the brain.
What is the most common cause of vertigo?
Benign Paroxysmal Positional Vertigo (BPPV) is the most common cause of vertigo, which is a symptom of the condition. Though not fully understood, BPPV is thought to arise due to the displacement of otoconia (small crystals of calcium carbonate) from the maculae of the inner ear into the fluid-filled semicircular canals. These semicircular canals are sensitive to gravity and changes in head position can be a trigger for BPPV. The posterior canal is the most commonly affected site, but the superior and horizontal canals can be affected as well. It should be noted that the superior canal is sometimes also referred to as the anterior canal and the horizontal canal is sometimes referred to as lateral canal.
How long does nystagmus last in BPPV?
Latency of onsent: there is a 5-10 second delay prior to onset of nystagmus. Nystagmus lasts for 5-30 seconds.
How does the vestibular system work?
The vestibular system monitors the motion and position of the head in space by detecting angular and linear acceleration. The 3 semicircular canals in the inner ear detect angular acceleration and are positioned at near right angles to each other. Each canal is filled with endolymph and has a swelling at the base termed the ampulla. The ampulla contains the cupula, a gelatinous mass with the same density as endolymph, which in turn is attached to polarized hair cells. Movement of the cupula by endolymph can cause either a stimulatory or an inhibitory response, depending on the direction of motion and the particular semicircular canal. There is a vestibular apparatus within each ear so under normal circumstances, the signals being sent from each vestibular system to the brain should match, confirming that the head is indeed rotating to the right, for example.
How long does BPPV last?
The signs and symptoms of BPPV are often transient, with symptoms commonly lasting less than one minute (paroxysmal). Episodes of BPPV can resolve after a few weeks or months, but may reappear at a later time. Signs and symptoms may include:
Question
I've been performing Semont and Epley procedures for 10 years with great success and I have a strong understanding of the differences between canal vs. cupulolithiasis.
Answer
There are several rare variants of BPPV which may occur spontaneously or subsequent to, canalith repositioning therapy in confirmed cases of posterior canal BPPV.
